Download to read offline
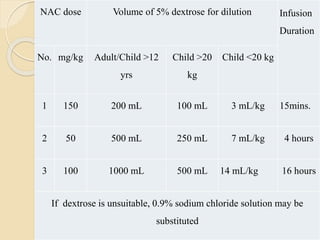

The document discusses paracetamol toxicity, its widespread use, overdose mechanisms, and treatment protocols. Paracetamol can cause severe hepatic damage when overdosed, with symptoms evolving from mild nausea to fatal liver necrosis due to toxic metabolites. Treatment includes supportive care, activated charcoal, and N-acetylcysteine (NAC), which is highly effective if administered early, alongside necessary monitoring for hepatic function.