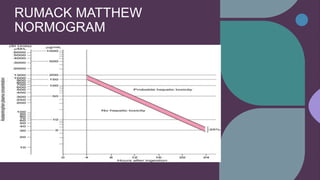
This document discusses acetaminophen (paracetamol) poisoning. It notes that acetaminophen toxicity is a common cause of liver transplantation worldwide. It reviews the etiology, evaluation, and treatment of acetaminophen overdose, including the use of N-acetylcysteine to prevent liver damage if administered within 8 hours of ingestion. It also discusses the Rumack-Matthew nomogram for assessing toxicity based on acetaminophen blood levels and time since ingestion. Complications of overdose can include liver failure and damage to other organs.

























![Parkinson's Disease [Advanced Pharmacology]](https://cdn.slidesharecdn.com/ss_thumbnails/07-210419085948-thumbnail.jpg?width=640&height=640&fit=bounds)












































