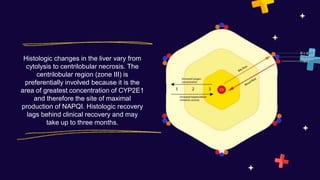
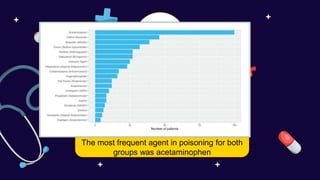
A 27-year-old male presented to the emergency department with vomiting, abdominal pain, altered mental status, and malaise. Many empty drug bottles were found in his bedroom. Toxicology testing did not find an overdose but acetaminophen toxicity was suspected due to the patient's recent depression and use of over-the-counter drugs. Acetaminophen toxicity can cause liver damage and is a common cause of acute liver failure in both the US and Saudi Arabia. Early identification and treatment with N-acetylcysteine can prevent liver injury if started soon after overdose.






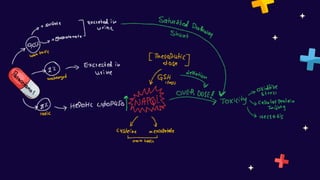
![1- Excessive intake (mc)
2- delay in treatment
3- Excessive CYP450 activity .
4-Decrease capacity of glucurnidation & sulfation
5- depletion of glutathione stores
Factor’s influence toxicity
Acute Alcohol ingestion Chronic Alcohol ingestion
protective by competing w
for CYP2E1 = decreasing
the amount of NAPQI
produced.
(18 or more standard alcoholic drinks [250 mg/dL])
increases the activity of CYP2E1
activity and depletes glutathione
stores and synthesis(in overdose
therapeutic dose .](https://image.slidesharecdn.com/paracetamoltoxicity-230622074123-1950d873/85/Paracetamol-toxicity-pptx-12-320.jpg)