

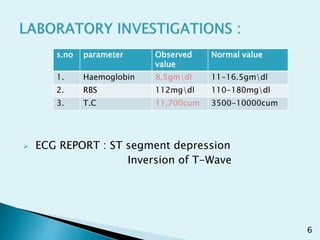
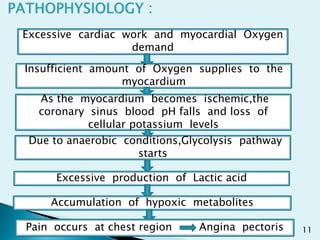
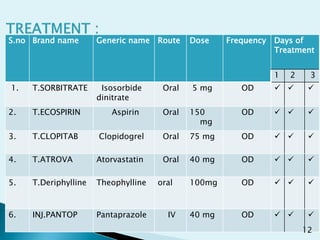



A 63-year-old male patient presented with chest pain, chest tightness, and shortness of breath. Based on his symptoms and ECG findings of ST segment depression and T-wave inversion, he was diagnosed with angina pectoris. He was treated with medications including isosorbide dinitrate, aspirin, clopidogrel, atorvastatin, pantoprazole, and theophylline. After three days of treatment, his condition was stable and he was discharged home with medications and lifestyle advice to control his cardiovascular risk factors.























































































