Downloaded 17 times
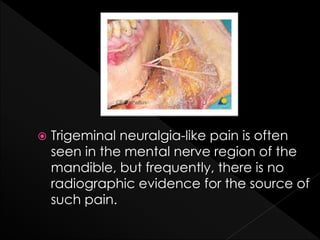







The document discusses trigeminal neuralgia-like pain related to the mental nerve, often with no identifiable radiographic source. It presents a case of an 88-year-old female with unexplained left jaw pain that was resolved temporarily with a diagnostic anesthetic block, leading to a diagnosis of atypical trigeminal neuralgia. Treatment options include medication and surgical interventions, although the success of medication is variable and surgical options are reserved for severe cases unresponsive to medical management.
















































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)

