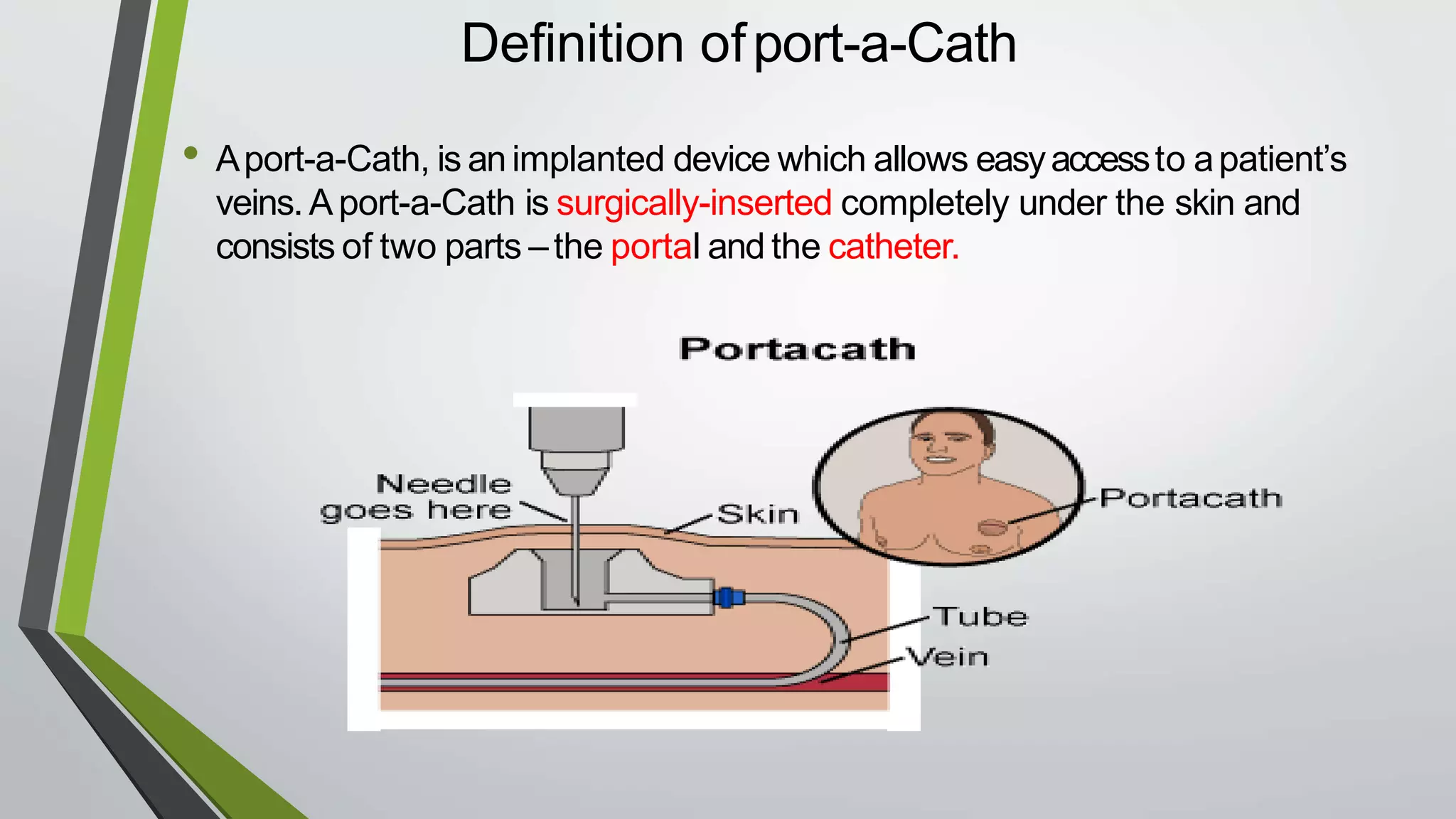
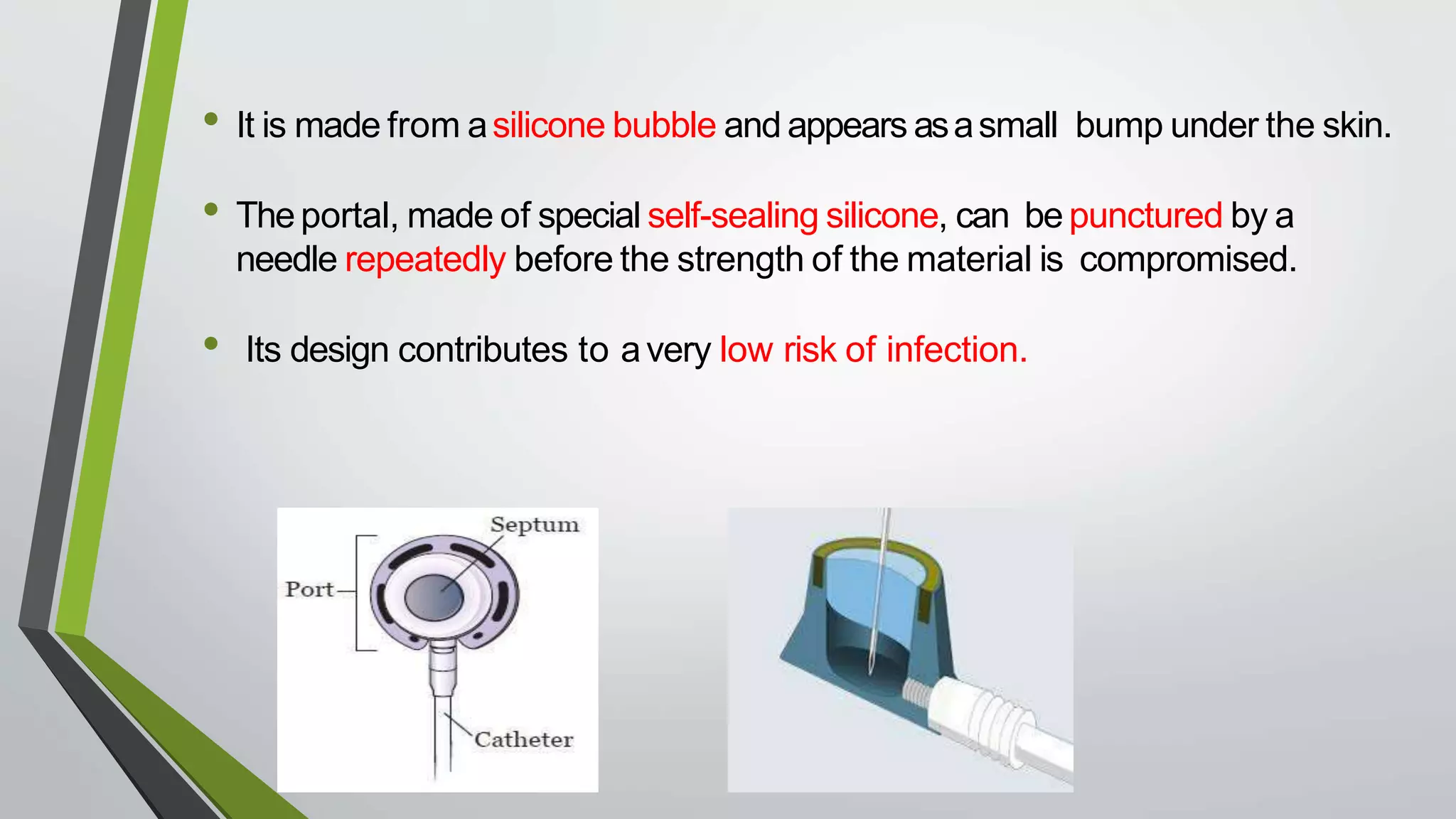
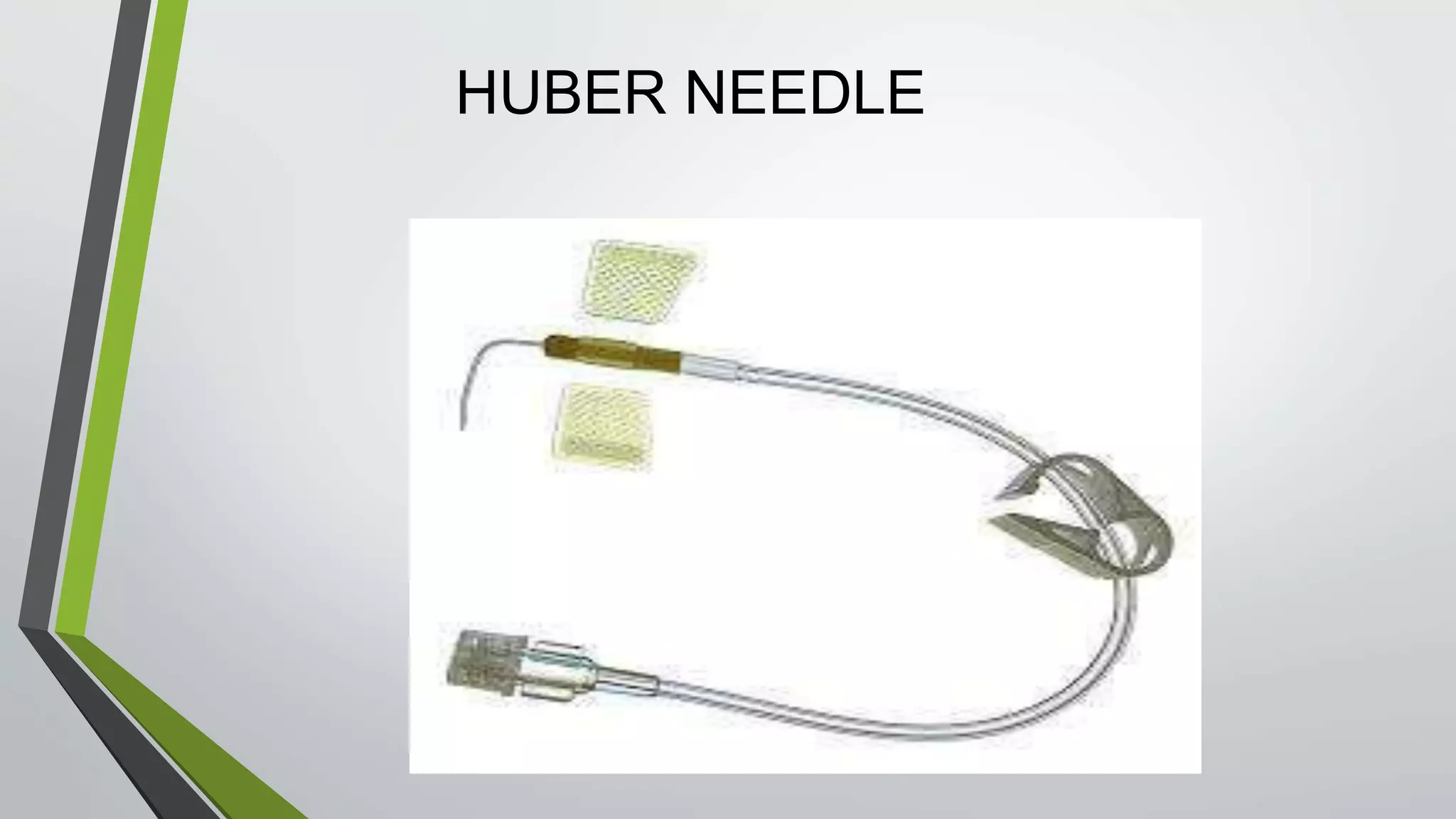
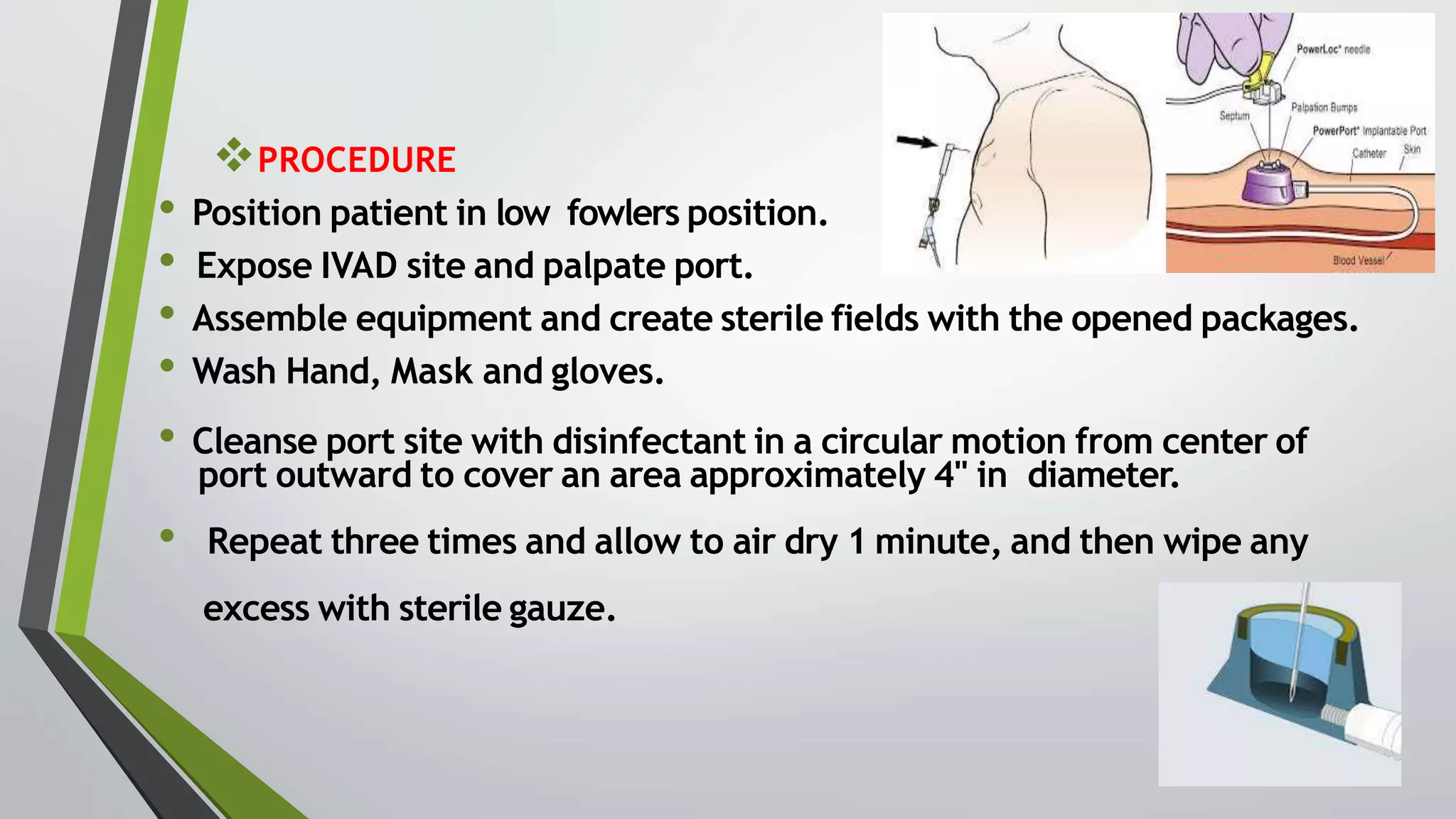
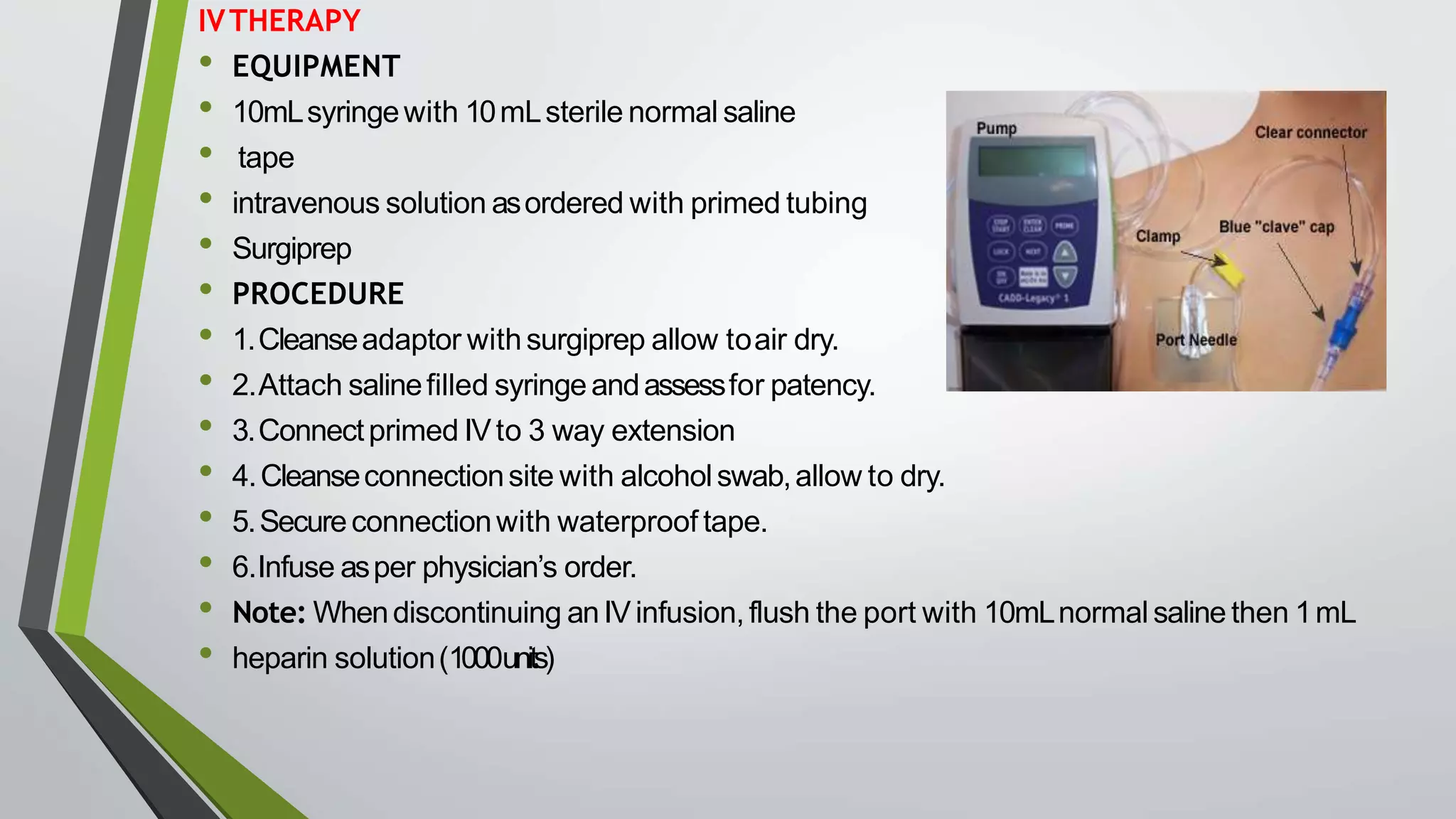
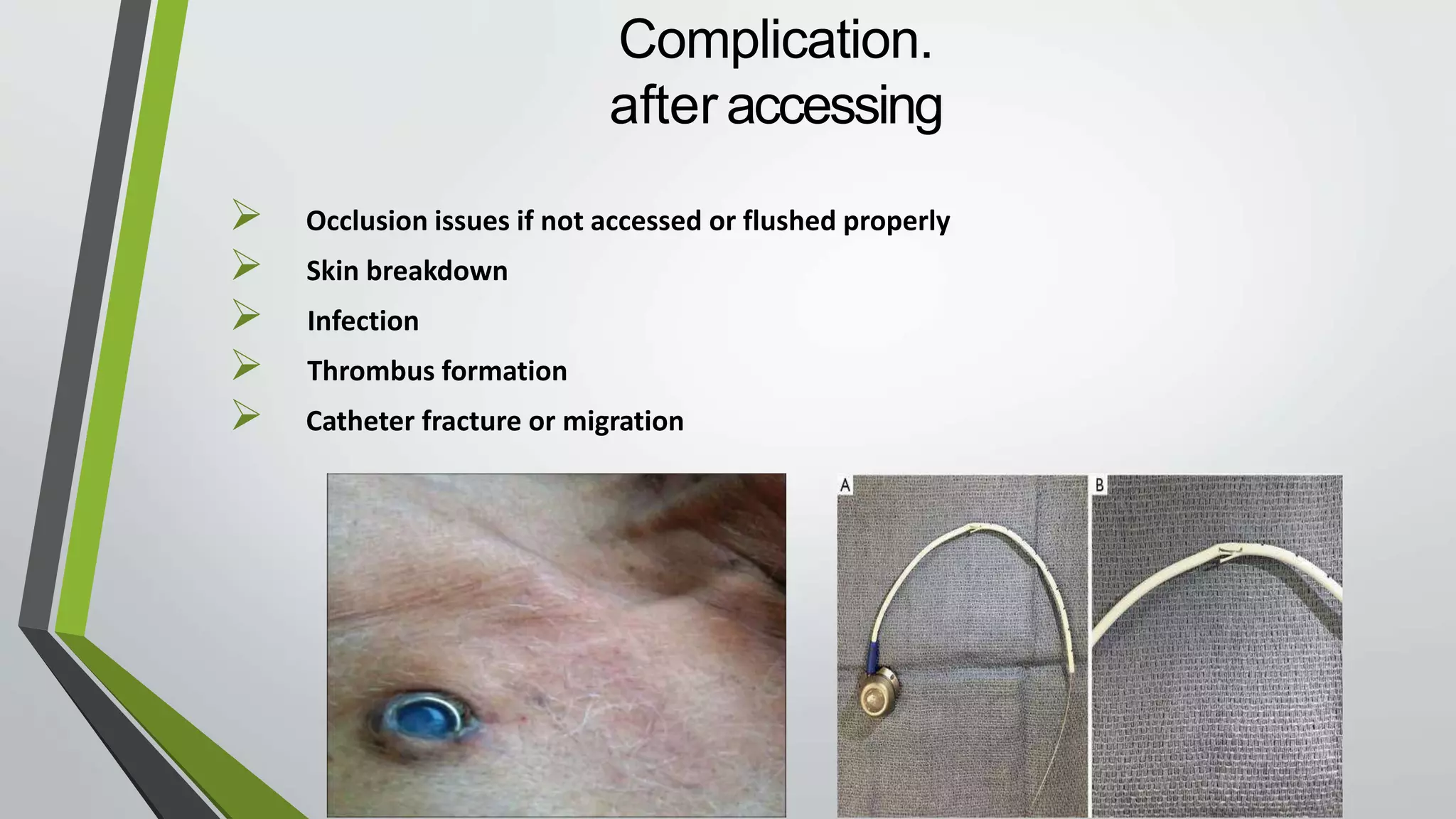
This document provides information on the care and use of a chemoport or port-a-cath. A port-a-cath is a surgically implanted device that provides long-term intravenous access. It consists of a portal and catheter under the skin. The portal can be punctured repeatedly by a Huber needle to administer medications, blood draws, or IV fluids. The document outlines the proper procedures for accessing the port with a needle, locking it with heparin, taking blood samples, starting IV therapy, and removing the needle. It also lists equipment needed and potential complications to watch for like infection, occlusion, or skin breakdown.