Downloaded 31 times
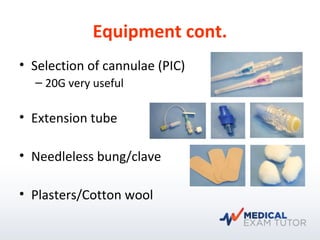
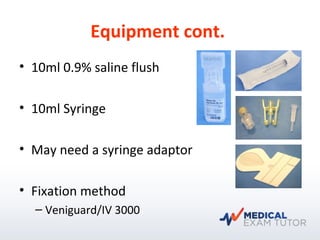
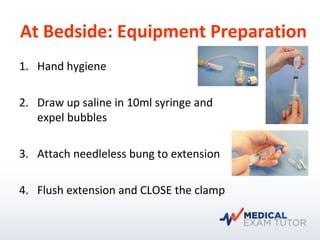
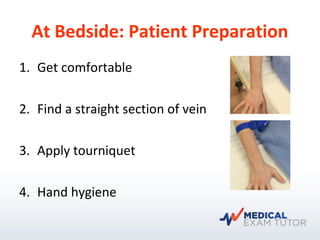



The document is a tutorial guide on intravenous cannulation aimed at interns, detailing equipment selection, patient preparation, and procedural steps. It emphasizes the importance of hand hygiene, proper equipment preparation, and safety measures during the procedure. Additionally, it addresses common FAQs regarding vein selection, cannula sizing, and complications like infiltration.



































































