Downloaded 92 times
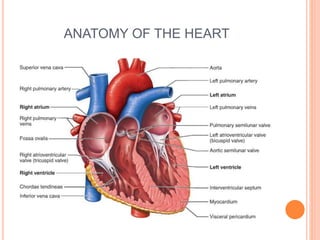

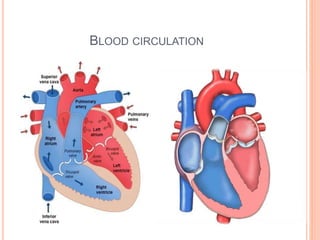


This document provides information on assessing cardiovascular health. It begins with an introduction noting cardiovascular disease is a leading cause of death. It then outlines the objectives which are to review cardiovascular anatomy and physiology, describe physical assessment, and review diagnostic procedures. The document proceeds to describe cardiovascular anatomy including the heart, circulation, and valves. It provides details on performing a cardiovascular assessment including taking a history, inspection, palpation, auscultation, and measuring blood pressure.