Downloaded 94 times




![Carcinoid Heart Disease
• a systemic disorder mediated by
elevated circulating levels of
vasoactive substances, including
serotonin (5-hydroxytryptamine
[5-HT]), 5-hydroxytryptophan,
histamine, bradykinin,
tachykinins, and prostaglandins
produced by a rare metastatic
neuroendocrine malignancy,
carcinoid
•
• Carcinoid syndrome is
characterized by a triad of
symptoms—flushing, diarrhea,
and bronchospasm—that occur
in association with hepatic
metastases](https://image.slidesharecdn.com/cardiomyopathy-170512071237/85/Cardiomyopathy-52-320.jpg)


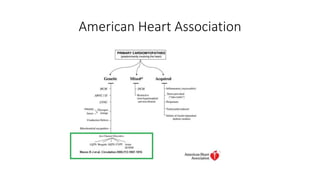
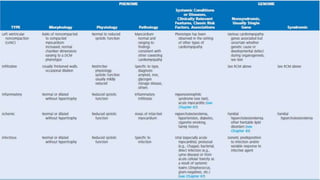
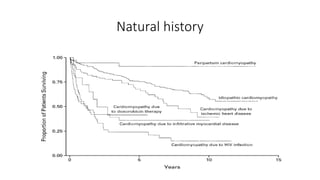
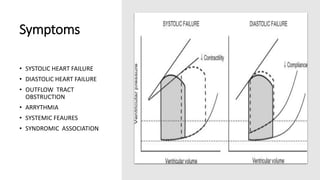
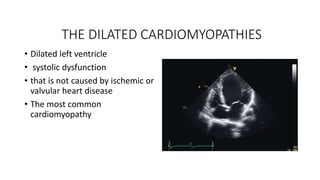
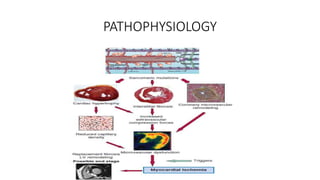
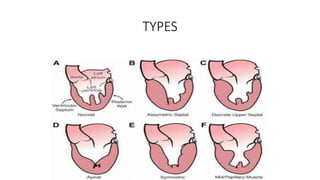
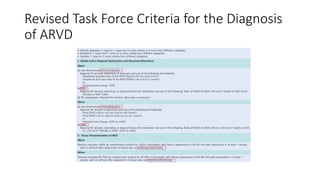
The document discusses various forms of cardiomyopathy, their definitions, classifications, symptoms, and complications. It encompasses types such as dilated, hypertrophic, restrictive, and arrhythmogenic right ventricular dysplasia, detailing pathophysiology, risk factors, diagnostics, and treatment options. Additionally, it covers associated conditions like carcinoid heart disease and long QT syndrome, highlighting the importance of genetic factors and the clinical implications of these heart muscle diseases.























































































