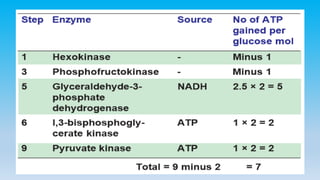
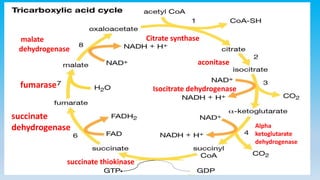
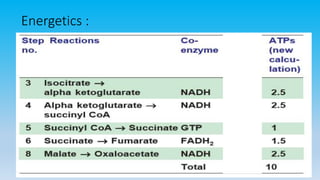
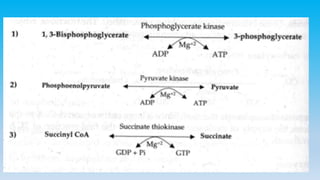
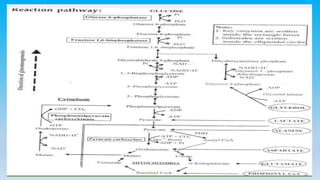
Glycolysis is the breakdown of glucose to pyruvate with production of energy. It occurs in the cytoplasm and can proceed with or without oxygen. Glycolysis is regulated by energy requirements of the cell and key enzymes. The citric acid cycle is the final common pathway for oxidation of acetyl CoA derived from carbohydrates, lipids, and proteins. It occurs in mitochondria and produces carbon dioxide, water, and energy in the form of ATP and NADH. Glycogen is the storage form of glucose and its synthesis and breakdown are regulated by hormones to maintain blood glucose levels. Gluconeogenesis produces new glucose from non-carbohydrate sources in the liver. Hormones like insulin and glucagon











































![Carbohydrate metabolism final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/carbohydratemetabolismfinalautosaved-250929151656-3b0eb421-thumbnail.jpg?width=640&height=640&fit=bounds)






![Carbohydrate Metabolism lecture 1 (Glycolysis) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/carbohydratemetabolismlecture1glycolysisautosaved-250923051041-f5c76835-thumbnail.jpg?width=640&height=640&fit=bounds)



































