Downloaded 448 times
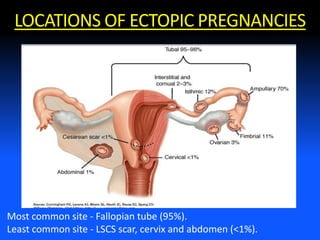
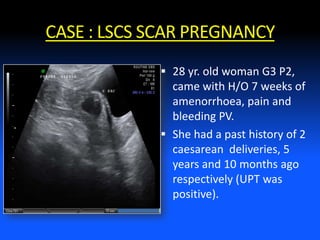

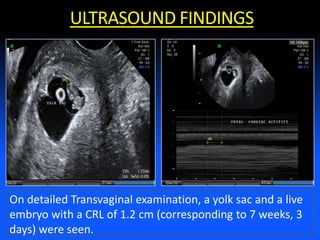

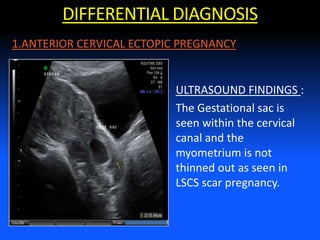
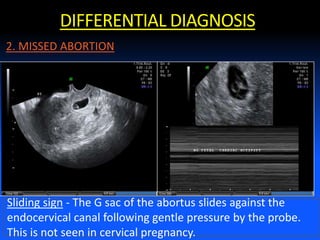
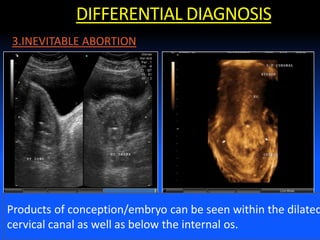



This case report describes a caesarean scar ectopic pregnancy in a 28-year old woman with two previous caesarean deliveries. Ultrasound found the gestational sac located in the lower uterine segment within the region of the previous caesarean scar. 3D imaging confirmed these findings. The differential diagnosis considered cervical ectopic pregnancy and missed abortion but color Doppler showed peripheral flow around the sac, confirming a caesarean scar ectopic pregnancy. Early detection of caesarean scar ectopic pregnancies by ultrasound is important to reduce risks of complications like hemorrhage which can require emergency hysterectomy.























































































