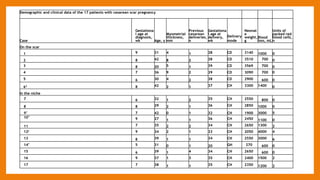
This study compared outcomes of cesarean scar pregnancies (CSP) implanted on the scar versus in the niche. Of 17 CSP cases, 6 were implanted on the scar and 11 in the niche. Those implanted on the scar had better outcomes: they did not develop morbidly adherent placenta and 5/6 delivered via c-section. Those implanted in the niche all developed morbidly adherent placenta and required hysterectomy, with 10/11 having placenta increta/percreta. CSP implanted in the niche may have worse outcomes than those implanted directly on the scar.



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















