Bangalore Call Girl Whatsapp Number 100% Complete Your Sexual Needs
Rcog2016.0b90285.normal
1. Combined Medical
& Surgical Management
Only One patient(7%) needed
hysteroscopy and surgical
evacuation of the uterus following
medical management, due to
the persistent retained Products
& ongoing vaginal bleeding.
CAESAREAN SCAR ECTOPIC PREGNANCY-A CASE SERIES
Dr Kausar Jabeen & Dr Jagadeeswari Karuppaswamy
Wrightington, Wigan and Leigh NHS Foundation trust
Introduction
Current prevalence of caesarean scar pregnancy is 1 per 2000 normal pregnancies
and 6 % of all the ectopic pregnancies in women with previous caesarean deliveries
(Rotas, Haberman and Levgur, 2006)
Early first trimester myometrial invasion in the case of scar implantation increases
the risk of uterine rupture, haemoperitoneum, hypovolemic shock, hysterectomy
and significant maternal morbidity and mortality (Seow et al., 2000 and Fylstra et
al., 2002).
Cervico-isthmic
Pregnancy
Spontaneous
Miscarriage
Cervico-isthmic
Pregnancy
Differential Diagnosis
• Empty uterine cavity
• Pregnancy lying
mainly in the cervix
• Characteristic
hourglass appearance
of the uterus due to
ballooned up cervical
canal.
• Gestational sac
lies low in the
uterine cavity.
• It is avascular
• Positive “sliding
organ sign
• Characterised by
absence of decidua
basalis
• Myometrial invasion
by trophoblast.
• Located essentially
within the uterine
cavity.
Audit
Objective: To examine the characteristics, management and outcomes of
caesarean scar ectopic pregnancies (CSPs) managed at Early
pregnancy assessment unit (EPAU)- Wrightington, Wigan and
Leigh NHS Foundation trust.
Duration: 3- 1/2 years period (Jan 2012- June 2015) Total cases: 15
Variables: Patients’ characteristics, gestation at diagnosis, management
& outcome
Diagnostic Criteria On Scan
Empty uterine cavity and cervical canal.
Gestational sac embedded in the myometrium
anterior to isthmic portion of the uterus.
Peritrophoblastic low impedance, high flow
circulation on colour and pulsed Doppler Examination.
Conservative: 08 (53%)
Medical (I/M Methotrexate) 06 (40%)
Medical & Surgical 01 (07%)
Conservative Management
Eight women (53%) were managed conservatively, as there was evidence
of spontaneous resolution.
Serial ultrasound and serum beta HCG levels were followed expectantly to
the resolution. Average diagnosis to complete resolution time was 33 days
(range: 21-63days).
S.N Age Number
of
Previous
CS
Presentation Initial Beta
HCG
Levels
Resolutio
n time
On scan
1 32yr 4 CS Misdiagnosed in TOP clinic as
Intra uterine pregnancy,
presented with persistent p/v
bleeding
< 0.2 mIU/ml 4 weeks
2 38yr 1 CS Misdiagnosed as miscarriage
and treated with vaginal
misoprostol. Persistent p/v
bleeding.
1251mIU/ml 9 weeks
3 28yr 1 CS P/V bleeding & pain 544 mIU/ml 3 weeks
4 30yr 2 CS P/V bleeding 1875 mIU/ml 7 weeks
5 29yr 1 CS P/V bleeding 188 mIU/ml 5 weeks
6 36yr 1 CS Misdiagnosed as tubal ectopic
pregnancy. Follow up scan
confirmed CSP
157 mIU/ml 6 weeks
7 39yr 1 CS P/V bleeding & pain 2988 mIU/ml 3 weeks
8 29yr 2 CS H/O recent CSP , P/V bleeding 403 mIU/ml 4 weeks
Case Summary -Conservative Management:
G3P2, Previous 2 CS. TVS- CS scar pregnancy (no delay in diagnosis)
Spontaneous resolution on serial scans. Declining β HCG:1875-1159-833-
502-47 (7-weks)
Spontaneous Resolution
Medical Management
Six women (40%) were treated with Intramuscular Methotrexate
injection (50mg/m2 body surface area).
Serum beta HCG levels were initially monitored on day-4 & day-7.
Ultrasound was performed weekly.
Once a decline in beta HCG levels was noted, weekly beta HCG
levels & ultrasound scan every 2-4 weeks until resolution were
performed.
S.N Age
Number
of
previous
CS
Presentation
Initial
Beta
HCG
levels
Number
of doses
Resolution
time
On scan
1 28yr 2 CS
P/V bleeding & pelvic
pelvic pain. Viable
CS scar pregnancy
on TVS
4673
mIU/ml
Two
Doses
20 weeks
2 29yr 1 CS P/V bleeding. Viable
Viable CS scar
pregnancy on TVS
16280
mIU/ml
Two
Doses
10 weeks
3 23yr 1 CS P/V bleeding &
pelvic pain.
35052
mIU/ml
Single
Dose
25 weeks
4 41yr 2 CS Ref by TOP clinic ?CS 38999
mIU/ml
Single
Dose
10 weeks
5 24yr 1 CS P/V bleeding, initially
initially misdiagnosed
misdiagnosed as
miscarriage.
32568
mIU/ml
Single
Dose
24 weeks
6 32yr 1 CS Misdiagnosed as
tubal ectopic
pregnancy on TVS.
CS scar pregnancy
confirmed on
laparoscopy.
20913
mIU/ml
Single
Dose
16 weeks
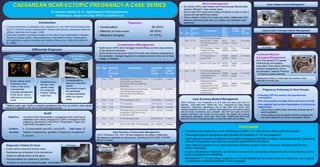
Case Summary-Medical Management
G3P2, Previous 1 CS. Presented in A & E with C/O pelvic pain and P/V
bleeding. Initial Beta HCG: 32000 mIU. TVS : Diagnosed as Tubal ectopic
pregnancy. Underwent Laparoscopy due to high beta HCG levels: Both
adnexae appeared normal & a vascular mass bulging from the anterior uterine
wall at the site of caesarean scar consistent with CSP was noted. No further
surgical intervention was carried out and patient was treated with systemic
methotrexate afterwards. Serial beta HCG levels: 32568-22063-9674-5449-
2283-492-230-38-14.Gradual resolution on USG was noted over 24 weeks.
Scan Images-medical Management
Laparoscopic Findings-medical Management
Pregnancy Following Cs Scar Ectopic
Following CSP five women had spontaneous
conceptions.
One of the patient amongst these had recurrent CSP.
Four patients had normal implantation of intrauterine
pregnancies.
One of them unfortunately had early fetal demise at 7
weeks gestation.
Three patients had successful full term pregnancies
and were delivered by elective caesarean section.
Conclusion
Caesarean scar pregnancy is a life threatening condition. It is more common than previously thought.
Transvaginal scan is emerging as gold standard for diagnosis of CS scar pregnancy.
High suspicion and early recognition of the salient sonographic findings is critical in directing treatment, preventing
maternal complications and allowing successful preservation of the uterus.
There does not appear to be a clear association between number of prior caesarean deliveries and CS scar
ectopic pregnancy.
An accurate selection of patients, an informed consent to the conservative treatment and a strict adherence to the
follow-up program are mandatory.
Management of CS scar ectopic pregnancy is not well established, but according to our experience, non surgical
(conservative & medical) treatment is very successful.
CS Ectopic
Retroverted Uterus Resolving CSP
Cs Ectopic
Misdiagnosed initially as miscarriage due to uterine cavity
distended with blood clots
Treatment
**Sliding organ sign: Ability to displace gestational sac from its position when gentle
pressure is applied on the cervix with transvaginal probe.
CS Ectopic
CS Ectopic
CS Ectopic
Normal Adnexa