Downloaded 82 times

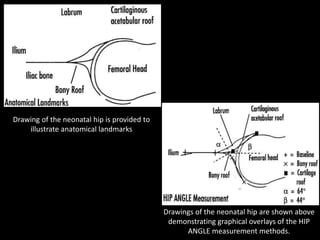
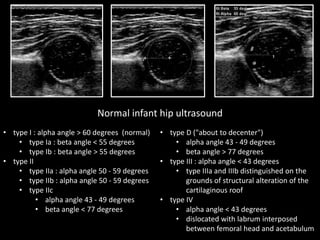
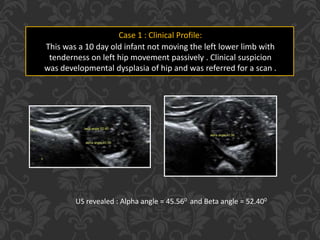
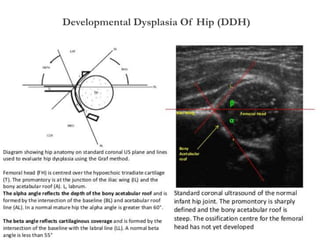
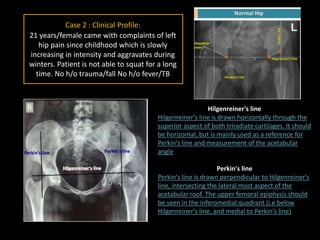
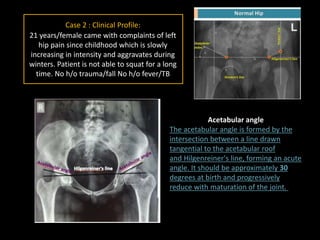
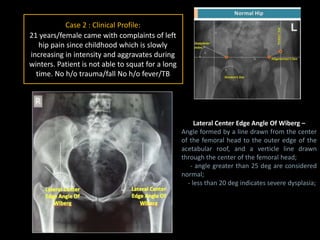
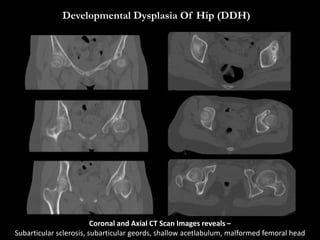
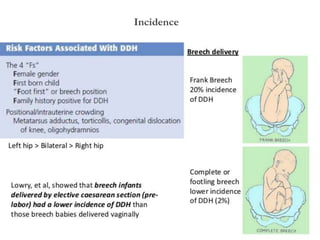
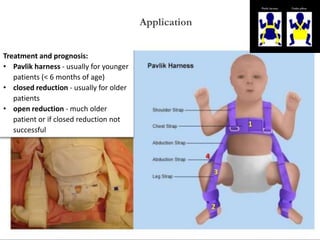

This document discusses developmental dysplasia of the hip (DDH). It defines DDH as an abnormal relationship between the femoral head and acetabulum, usually caused by ligamentous laxity or abnormal positioning in utero. The incidence is reported as 1.5 to 20 per 1000 births, with most abnormal hips resolving spontaneously within 2-8 weeks. Ultrasound images are presented to demonstrate measurement methods for classifying DDH. Two clinical cases are described. Treatment options including Pavlik harness, closed reduction, and open reduction are mentioned. References are provided at the end.





























































































