Downloaded 106 times

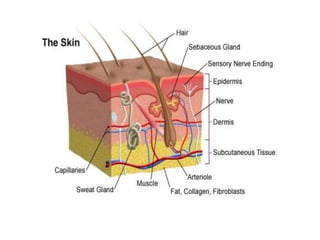
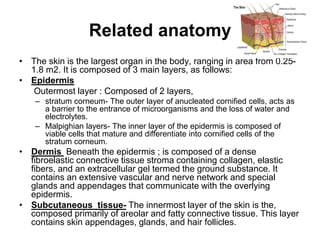
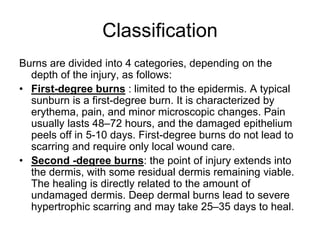

- The document discusses the anatomy, classification, pathophysiology, assessment, and management of pediatric burns. It describes the layers of the skin and how burns are classified based on depth. Management of minor burns involves debriding dead tissue, evaluating the wound, and applying semiocclusive dressings. Major burns require IV fluids and special attention to risks like hypothermia and fluid imbalance due to immature kidneys in young children.























































































