Downloaded 13 times





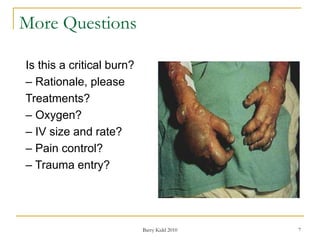










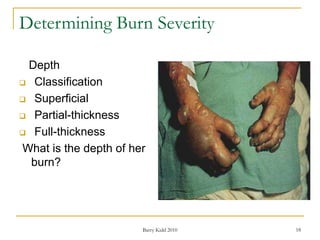



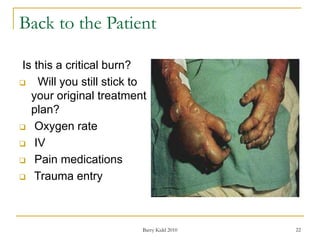


























This document discusses burn assessment and management. It provides details on assessing burn severity based on depth, percentage of total body surface area burned, and other factors. It also describes the mechanisms and potential complications of thermal, electrical, and inhalation burns. For the case study, the patient has partial thickness burns isolated to the lower arms, comprising less than 10% TBSA. While painful, this is not considered a critical burn based on the assessment criteria described in the document.























































































