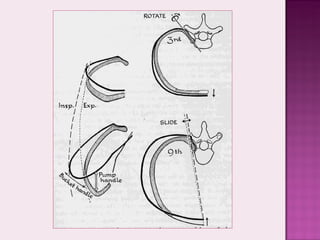
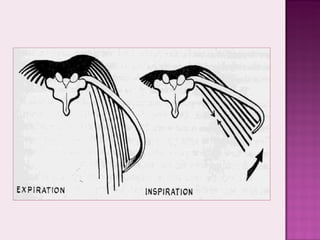
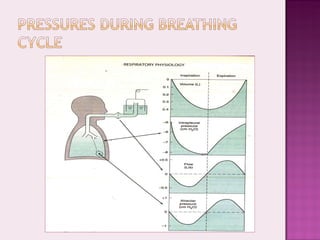
The document discusses the mechanics of breathing and factors that influence gas exchange in the lungs. It describes how the diaphragm and external intercostal muscles cause the chest cavity to expand and contract. This creates pressure differences that allow air to flow into and out of the lungs down a pressure gradient. Resistance to airflow is determined by properties of the airways like their size, branching patterns, and surface properties. Lung compliance and alveolar surface tension also impact gas exchange efficiency in the lungs.