Downloaded 344 times








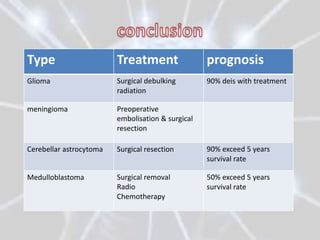


The document discusses different types of brain tumors, including gliomas, meningiomas, and medulloblastomas. It covers symptoms, risk factors, diagnosis methods like MRI and CT scans, and treatment options for brain tumors such as surgery, radiation therapy, chemotherapy, and managing increased intracranial pressure. The prognosis depends on the specific type of brain tumor, with some like glioblastoma multiforme having a very poor median survival rate.























































































