1) Growing skull fractures are rare fractures in children that enlarge over time due to dural laceration and brain pulsations.
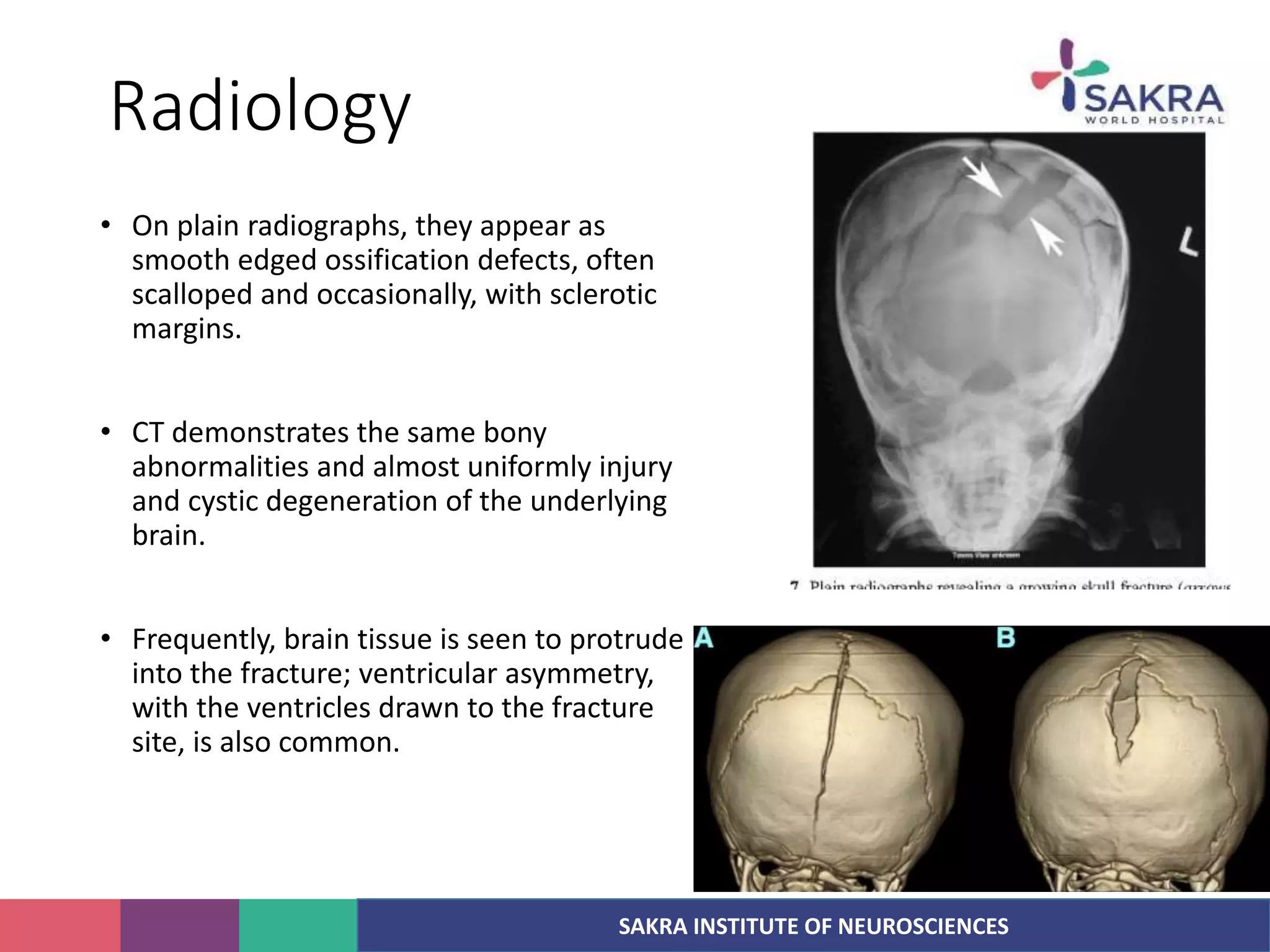
2) They typically present as a subgaleal fluid collection overlying a skull fracture in children under 3 years old with neurological deficits.
3) Treatment involves identifying the dural tear, repairing the dura, resecting herniated brain tissue, and covering the bone defect - often with a bone graft or synthetic material.