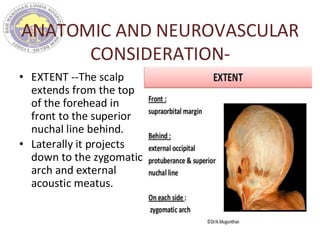
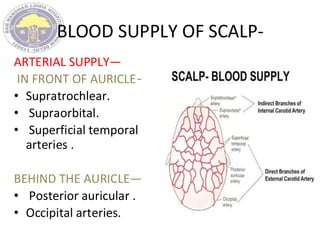
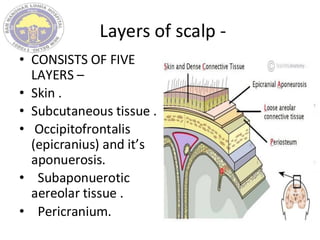
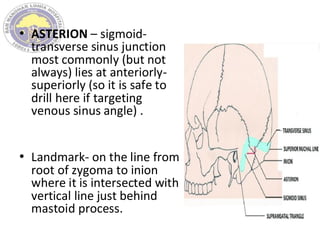
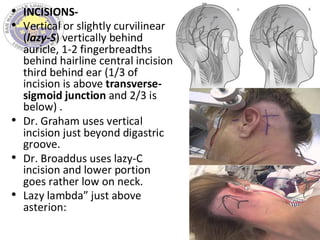
The document outlines the surgical procedures and considerations for craniotomy, detailing anatomical and neurovascular aspects, blood supply, and layers of the scalp. It describes various techniques for skin incisions, types of craniotomy, and specific approaches like the supraorbital keyhole craniotomy and temporal flaps, while emphasizing complications and perioperative management. Key principles include meticulous preparatory steps, proper patient positioning, and layered closure to ensure optimal outcomes.