Downloaded 412 times

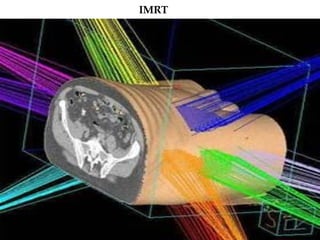

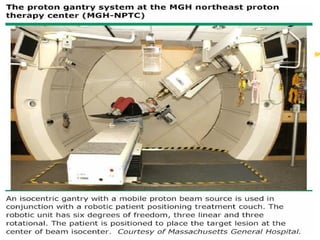


Radiation therapy plays an important role in the management of many bone tumors as an adjunct to surgery or as primary treatment for inoperable tumors. Newer radiation techniques like IMRT and proton beam therapy allow for more conformal dose distributions that improve local tumor control while reducing damage to surrounding healthy tissues. Radiation is used as primary treatment, post-operatively, or palliatively depending on the tumor type, location, surgical margins, and other factors.























































































