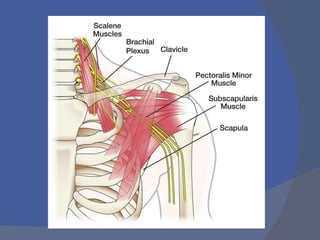
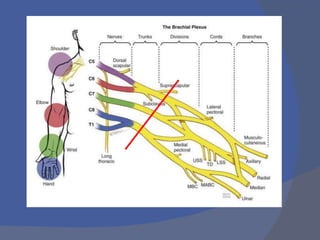
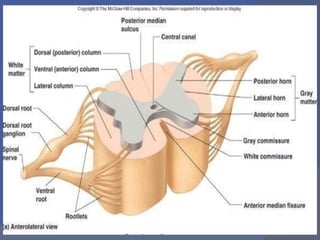
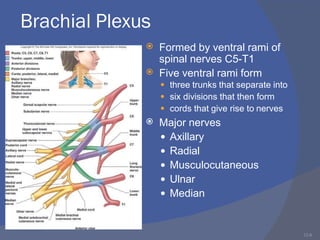
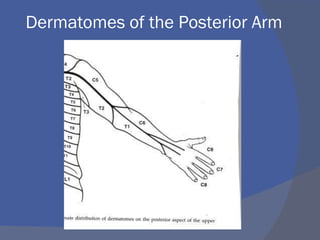
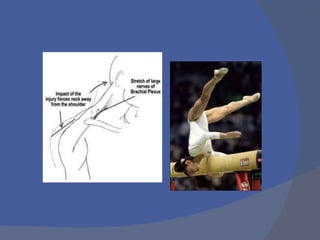
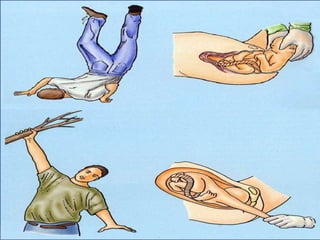
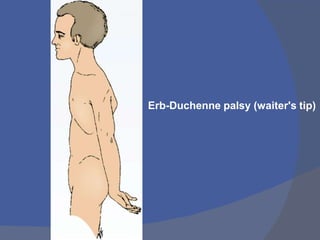
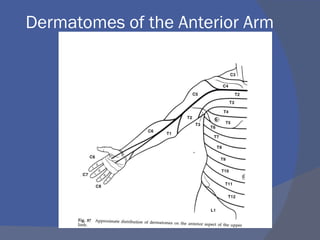
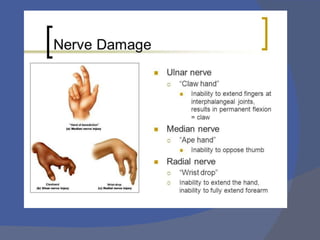
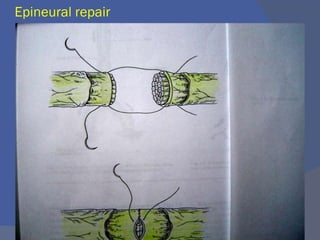
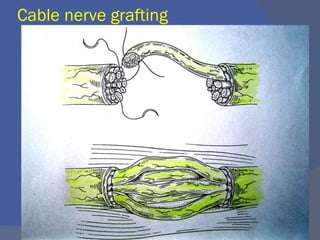
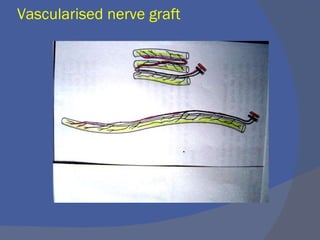
This document discusses brachial plexus injuries, including their etiology, diagnosis, and management. It provides details on the anatomy of the brachial plexus and its branches. Injuries are classified as upper (Erb's palsy) or lower (Klumpke's palsy) lesions. Diagnostic tests include imaging, EMG, and nerve conduction studies. Conservative management is used for neonatal injuries, while surgical options for adults include nerve grafting, transfers, and repairs. The document outlines various surgical techniques and notes advances in treating preganglionic injuries.