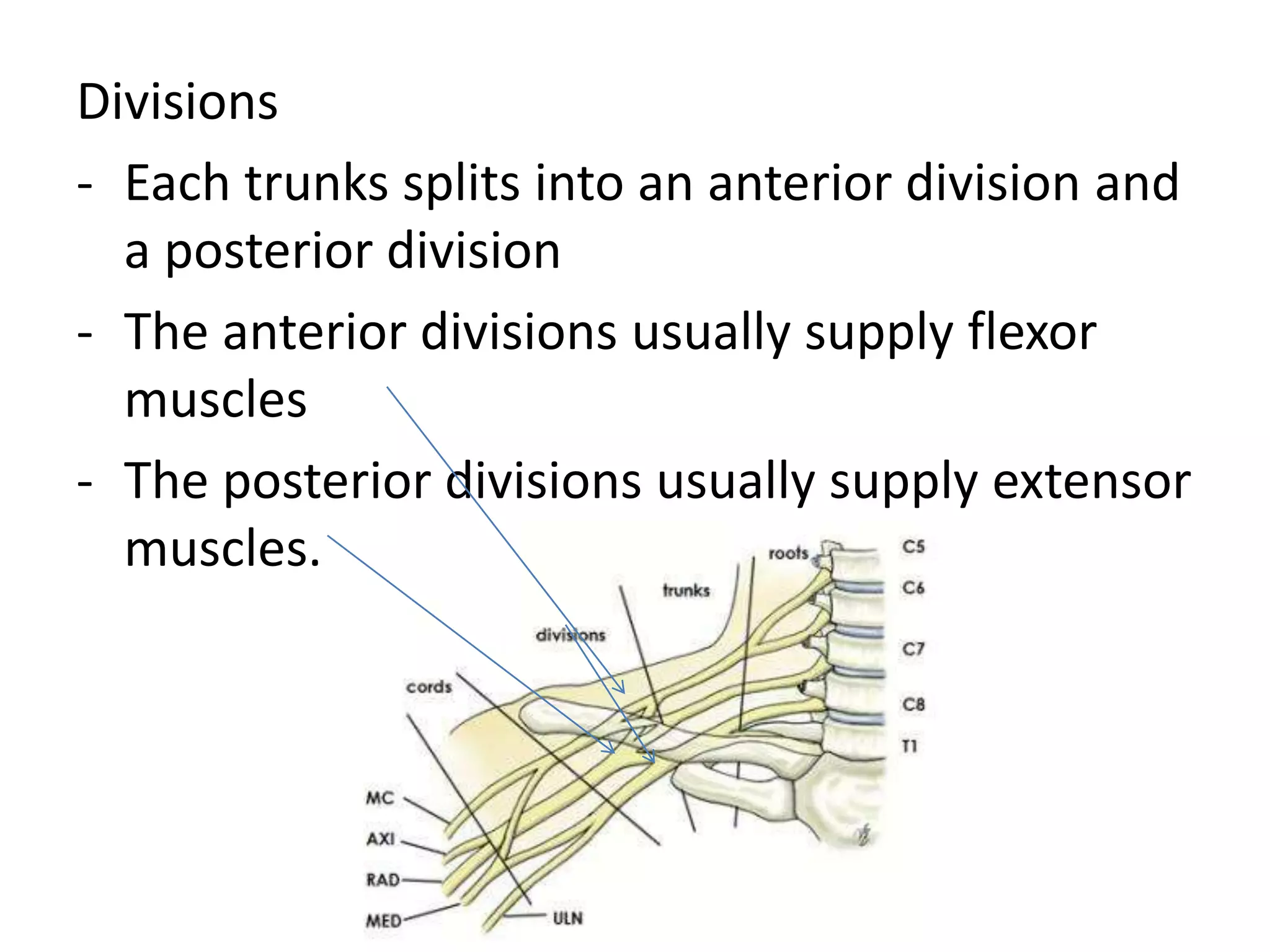
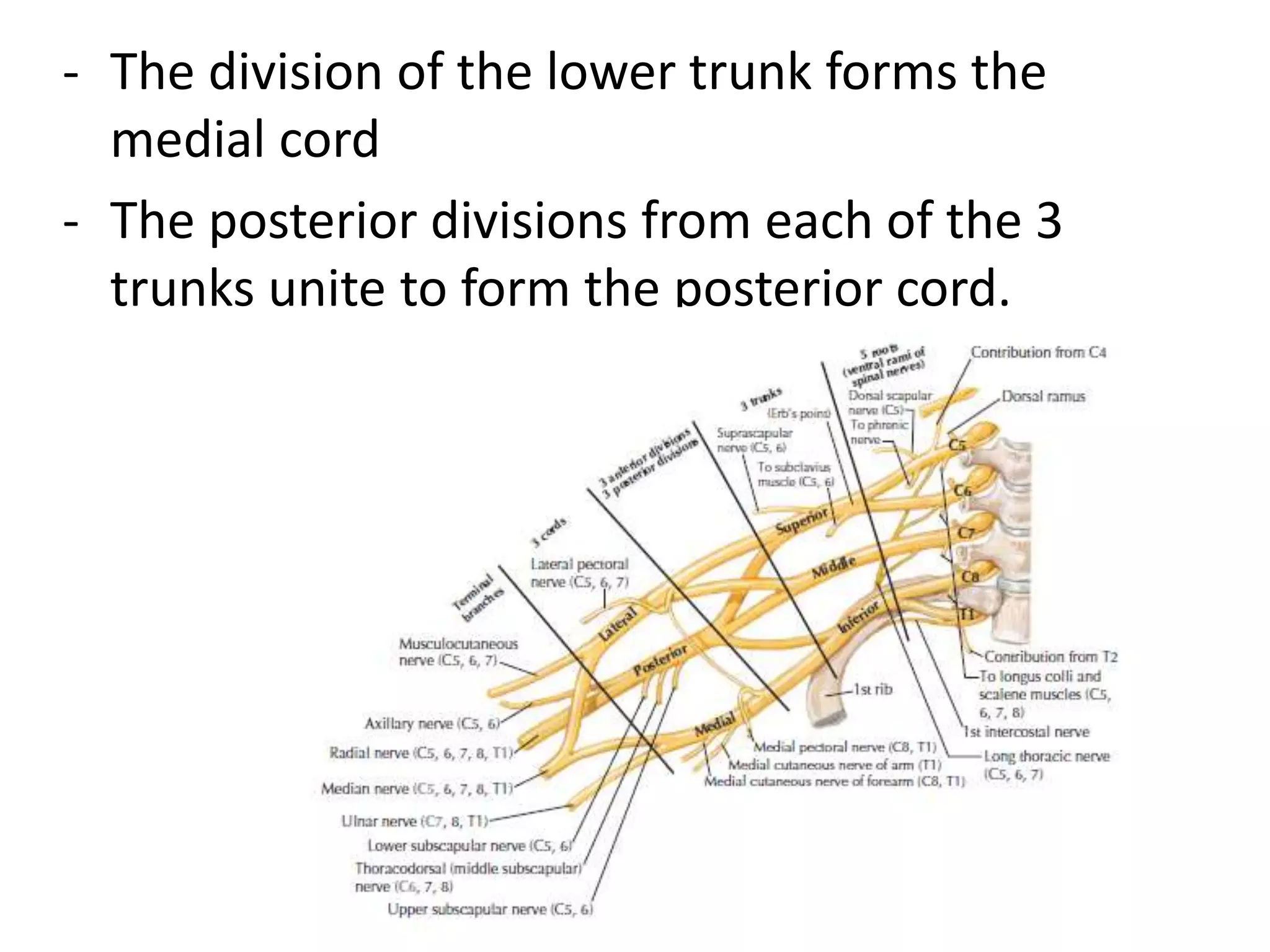
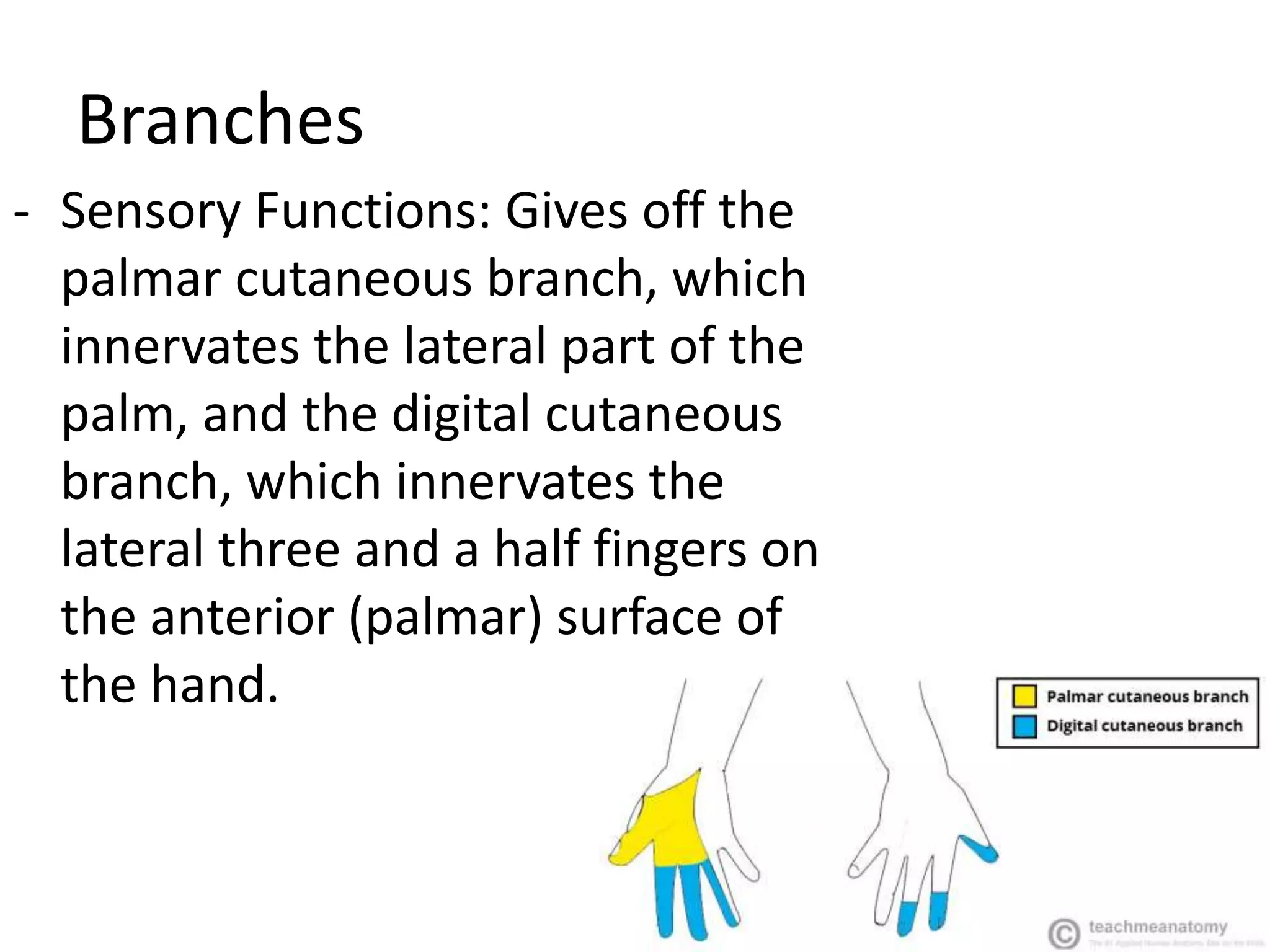
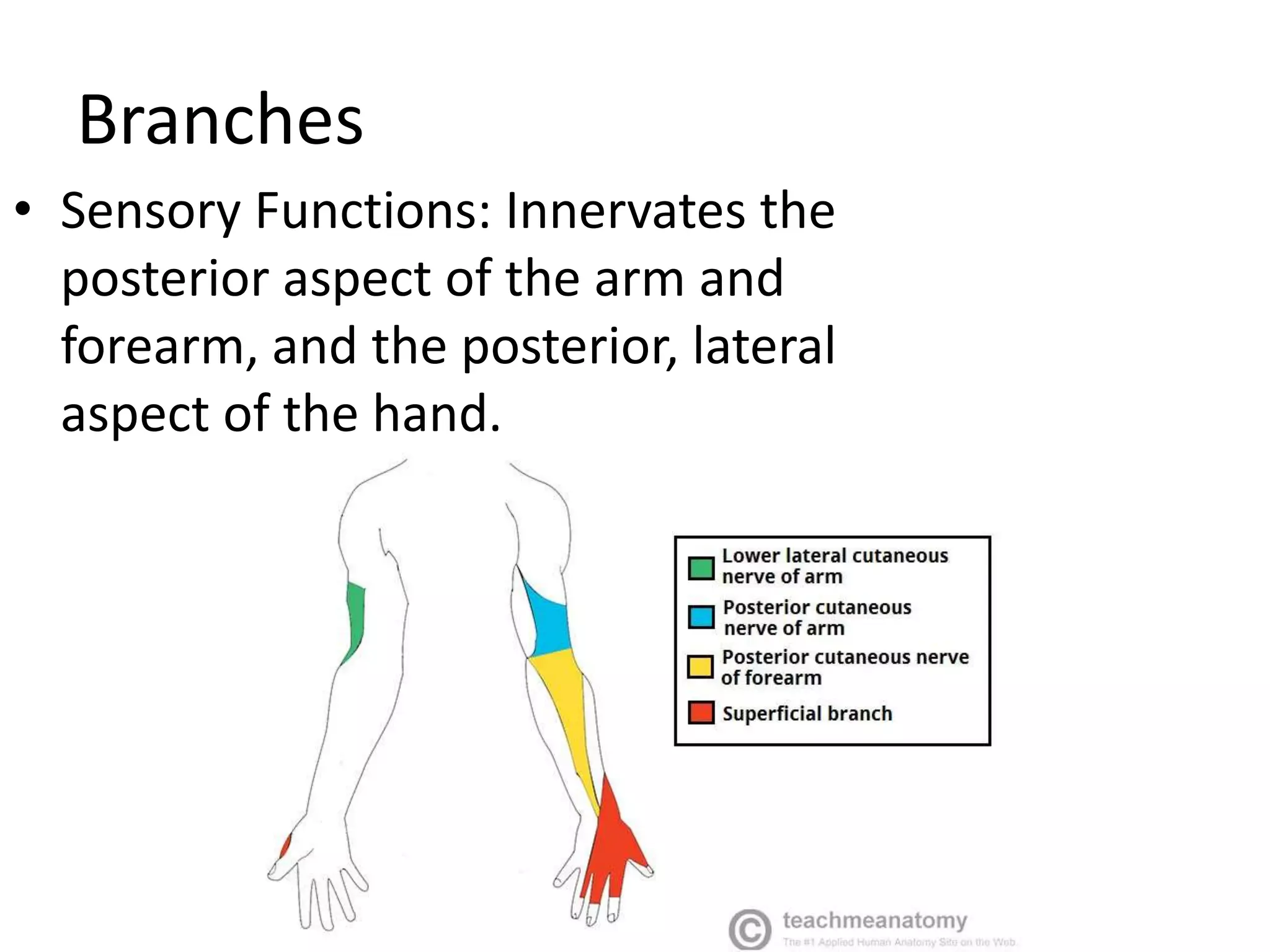
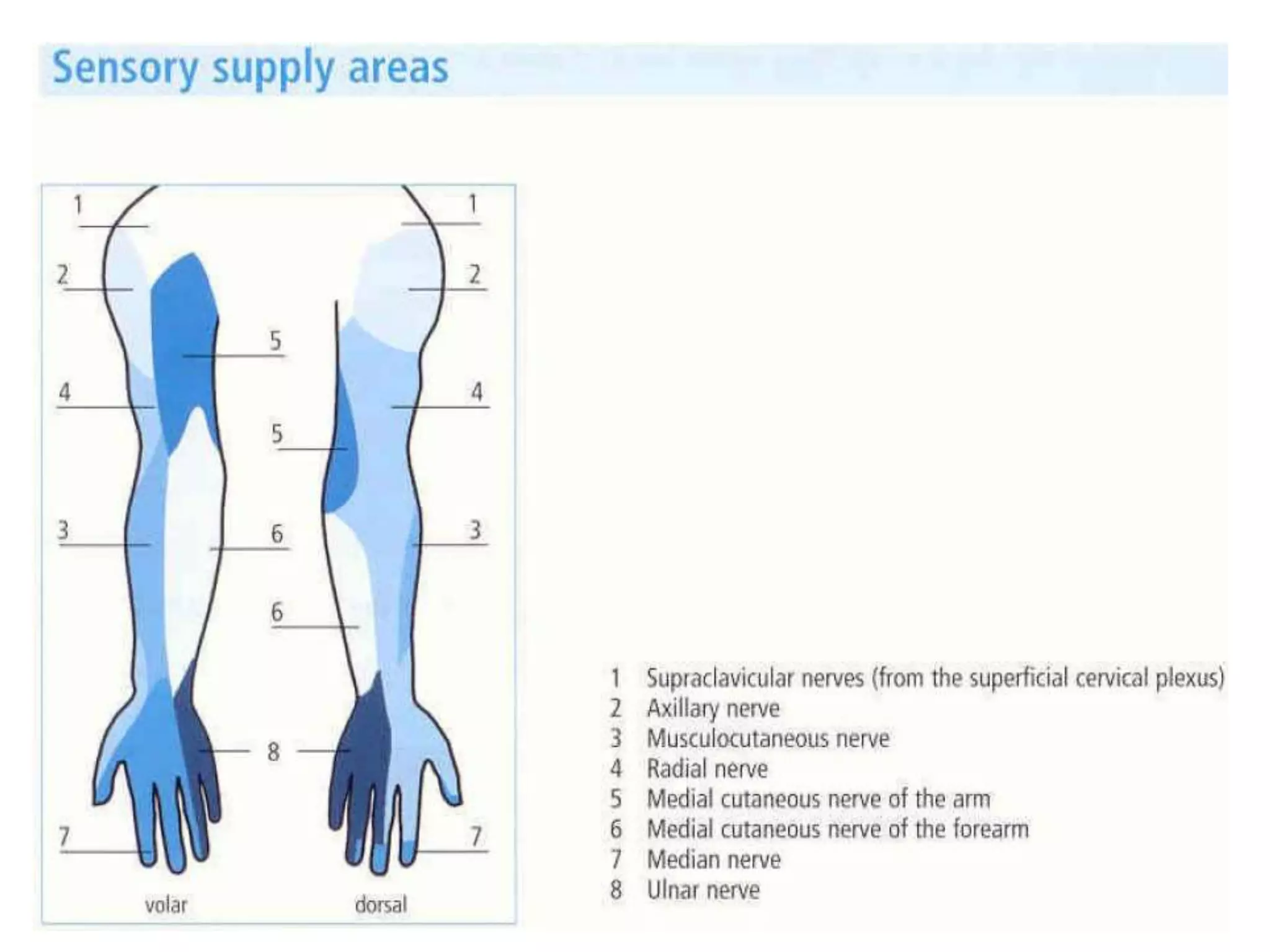
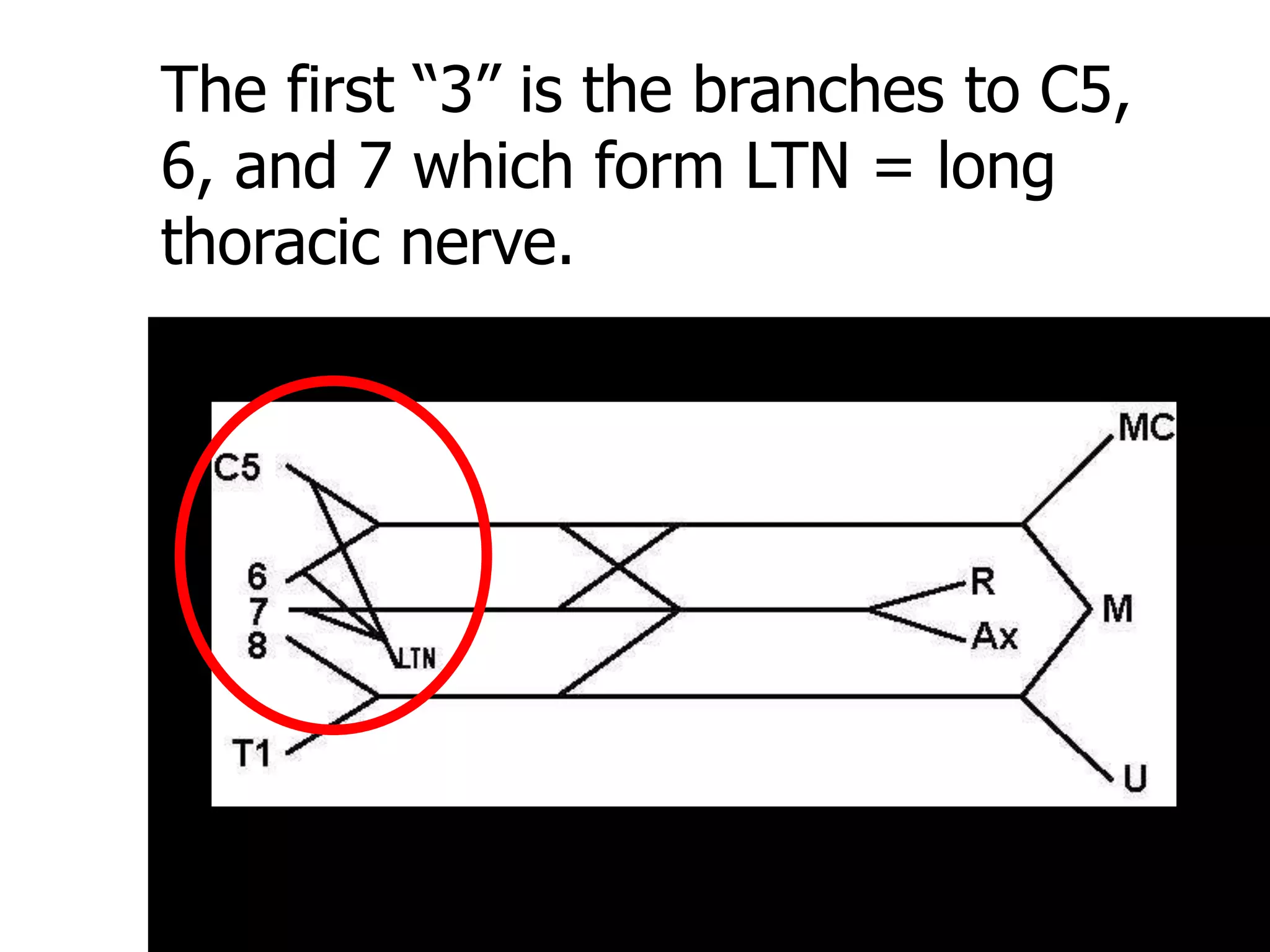
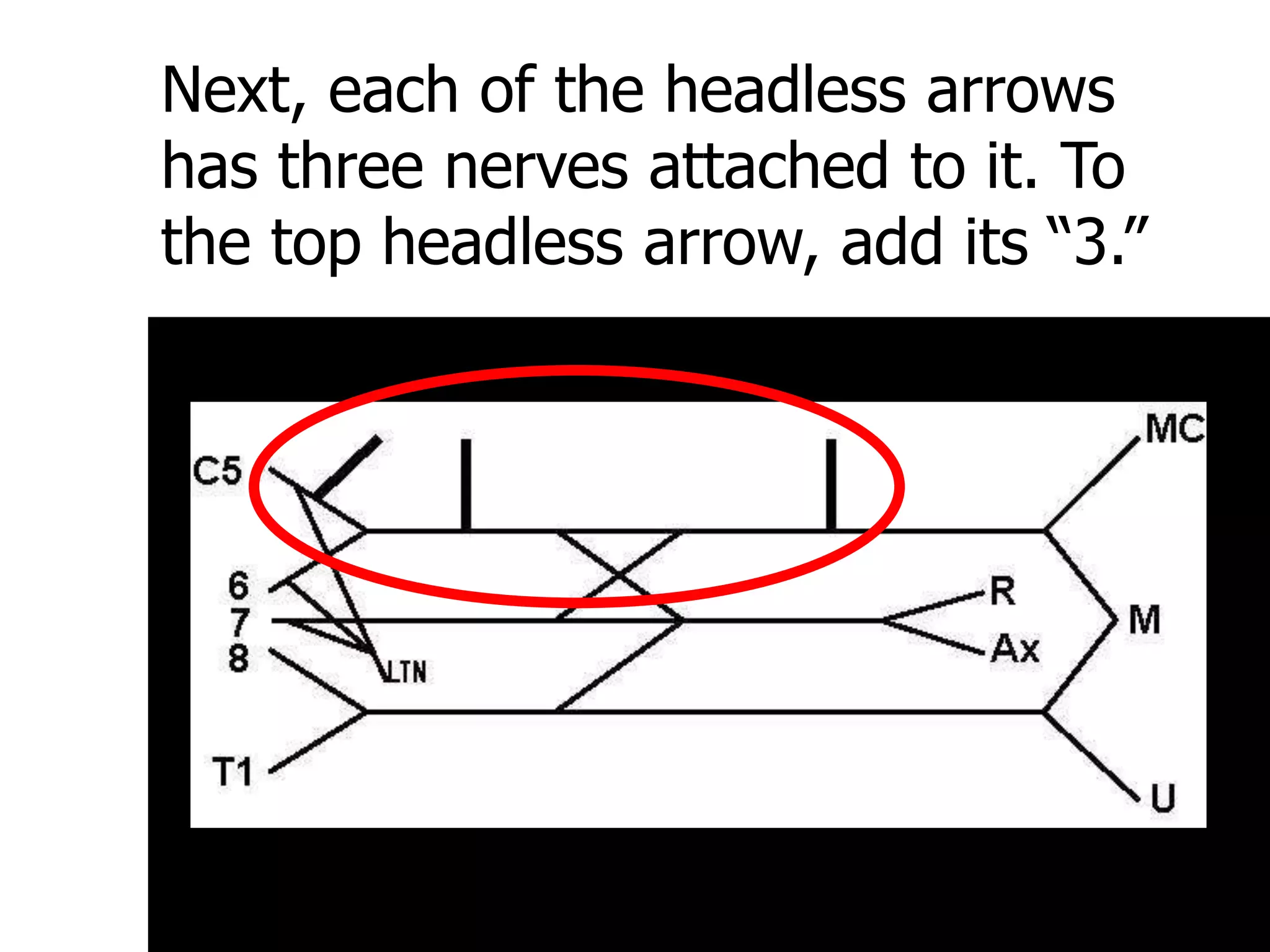
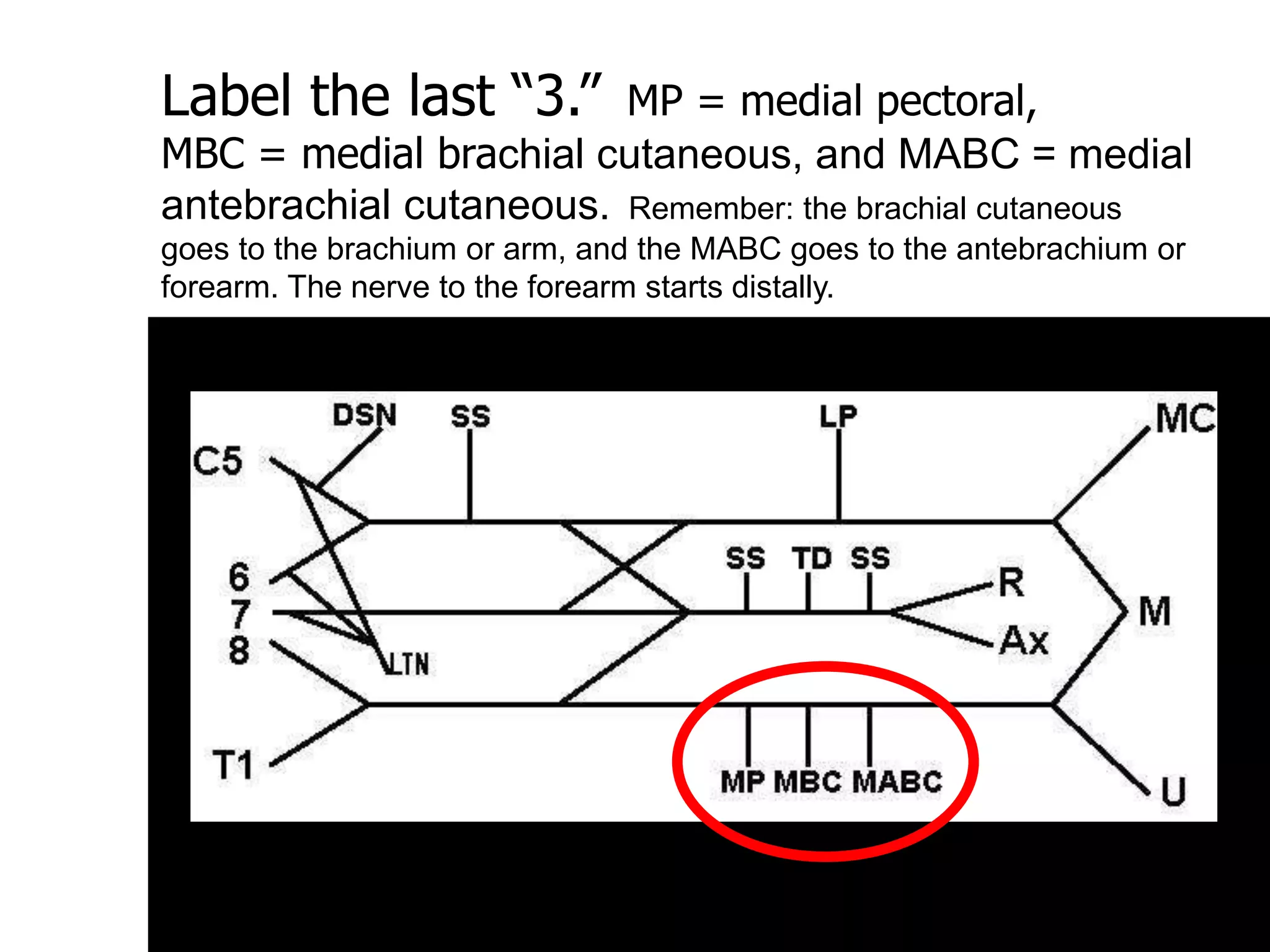
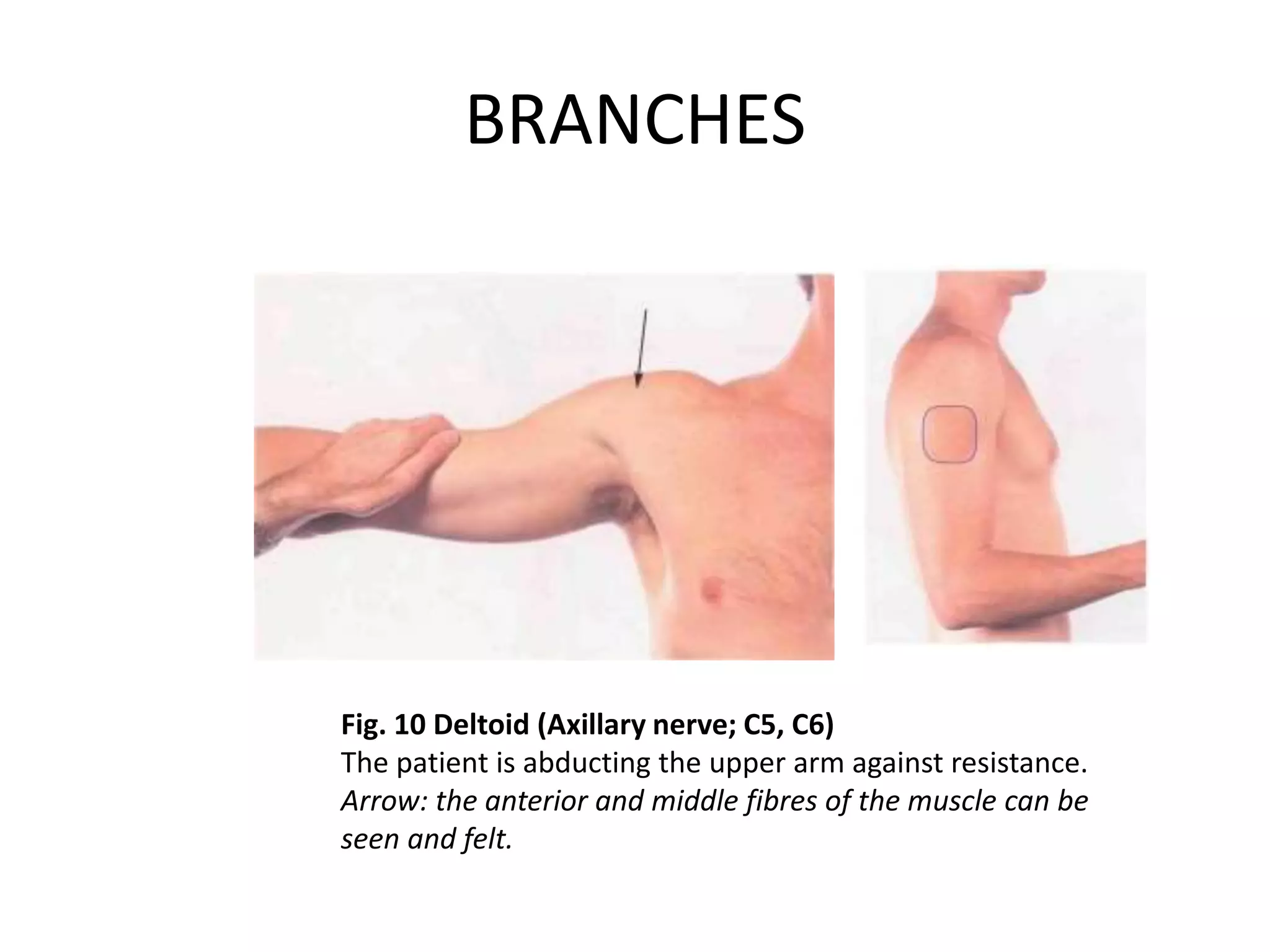
The brachial plexus is formed from the ventral rami of cervical and upper thoracic spinal nerves, which unite to form roots, trunks, divisions, cords, and branches that innervate muscles and skin of the upper limb. It is subdivided anatomically and each subdivision is associated with particular nerves, muscles, and cutaneous innervation. Injuries to different levels of the brachial plexus result in variable patterns of muscle denervation and functional impairment that require different surgical procedures.
















































































![Radiologic_Anatomy_of_the_Brachial_plexus [final].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicanatomyofthebrachialplexusfinal-250811175545-691d20d9-thumbnail.jpg?width=640&height=640&fit=bounds)

![1. brachial plexus & its applied anatomy[1]](https://cdn.slidesharecdn.com/ss_thumbnails/1-brachialplexusitsappliedanatomy1-100602035429-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

































