Downloaded 241 times

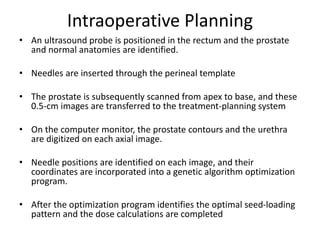
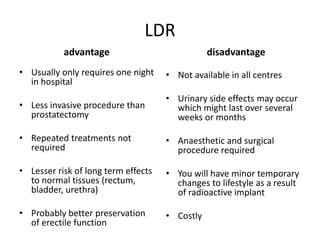
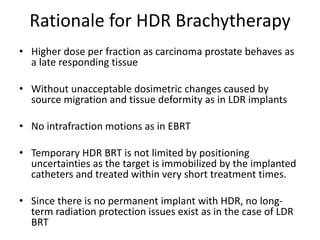
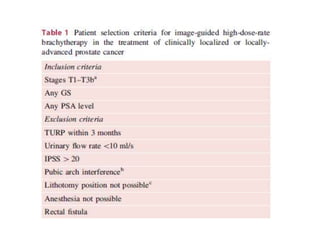


This document discusses brachytherapy for prostate carcinoma, detailing the techniques and history of low-dose rate (LDR) and high-dose rate (HDR) treatments. It outlines patient selection criteria, procedural steps, dosimetry considerations, potential advantages and disadvantages, and associated side effects such as urinary and rectal toxicity. The document also highlights factors influencing seed loss and emphasizes the importance of careful planning and post-procedure follow-up.




























































































