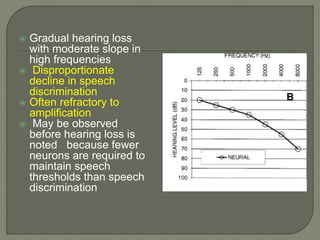
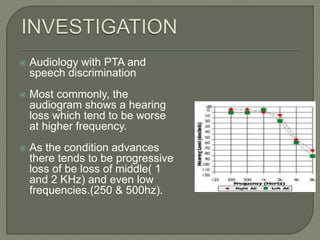
Presbycusis, or age-related hearing loss, is caused by a gradual degeneration of the inner ear and auditory nerve that commonly occurs in older adults over 60. It is a progressive, irreversible condition that results in difficulty hearing soft sounds and speech in noisy environments. The risk and severity of presbycusis increases with age and is influenced by factors like noise exposure, genetics, sex, and health issues. Treatment options focus on amplification with hearing aids and addressing any underlying health or lifestyle factors that may contribute to the condition.