
Downloaded 13 times

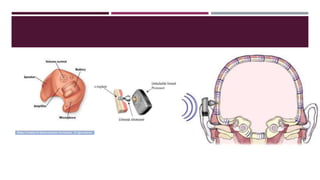
This document discusses principles for selecting amplification for children with hearing loss. It addresses choosing the routing of sound transmission via air conduction, bone conduction, or electrical stimulation. Bilateral amplification is generally recommended unless contraindicated. The style of hearing aid should consider factors like ear canal size and feedback risk, and BTEs are often preferred while the ear is growing. Earmold selection and replacement is important due to growth, and venting needs to avoid feedback while maintaining high frequencies. Safety concerns include batteries and volume controls.
















































![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)






































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)