Downloaded 170 times











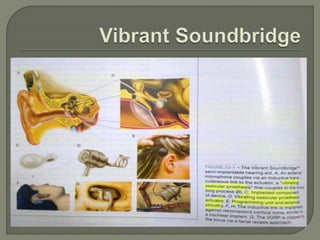











The document discusses middle ear implants as a type of hearing aid for patients with mild to severe hearing loss. It describes two main types of transducers used in middle ear implants - electromagnetic and piezoelectric. Several implant devices are discussed, including the Vibrant Soundbridge, Middle Ear Transducer (MET), Carina, and Esteem. Clinical trial results for some devices show significant improvement in functional gain and patient satisfaction compared to conventional hearing aids.



































































