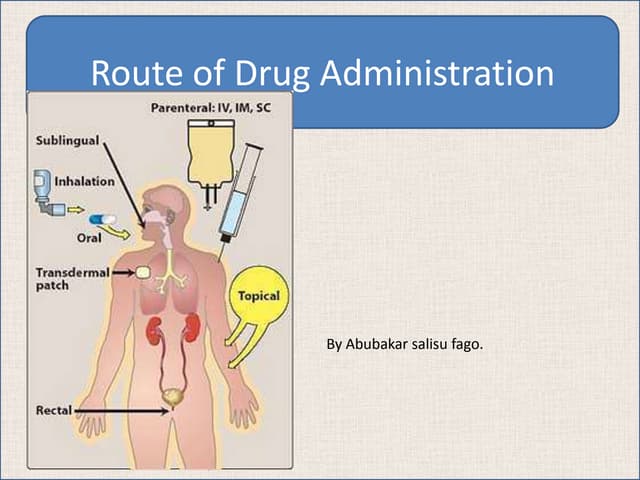
The document discusses various routes of drug administration including enteral (oral, buccal, rectal) and parenteral (injections like IV, IM, SC; topical, inhalation) routes. It provides details on factors affecting absorption for different routes like buccal/sublingual, rectal, intravenous, subcutaneous, intramuscular, inhalation, nasal and topical administration. Advantages and disadvantages of each route are highlighted with examples.



![Buccal/Sublingual Route Drug is taken as smaller tablets which are held in the mouth or under the tongue. Buccal tablets are often harder tablets [4 hour disintegration time], designed to dissolve slowly. Nitroglycerin, as a softer sublingual tablet [2 min disintegration time] may be used for the rapid relief of angina. This ROA is also used for some steroids such as testosterone and oxytocin. Nicotine containing chewing gum may be used for cigarette smoking replacement.](https://image.slidesharecdn.com/biopharmaceuticslecture42-100627180543-phpapp01/75/Biopharmaceutics-lecture4-2-4-2048.jpg)