Downloaded 36 times





























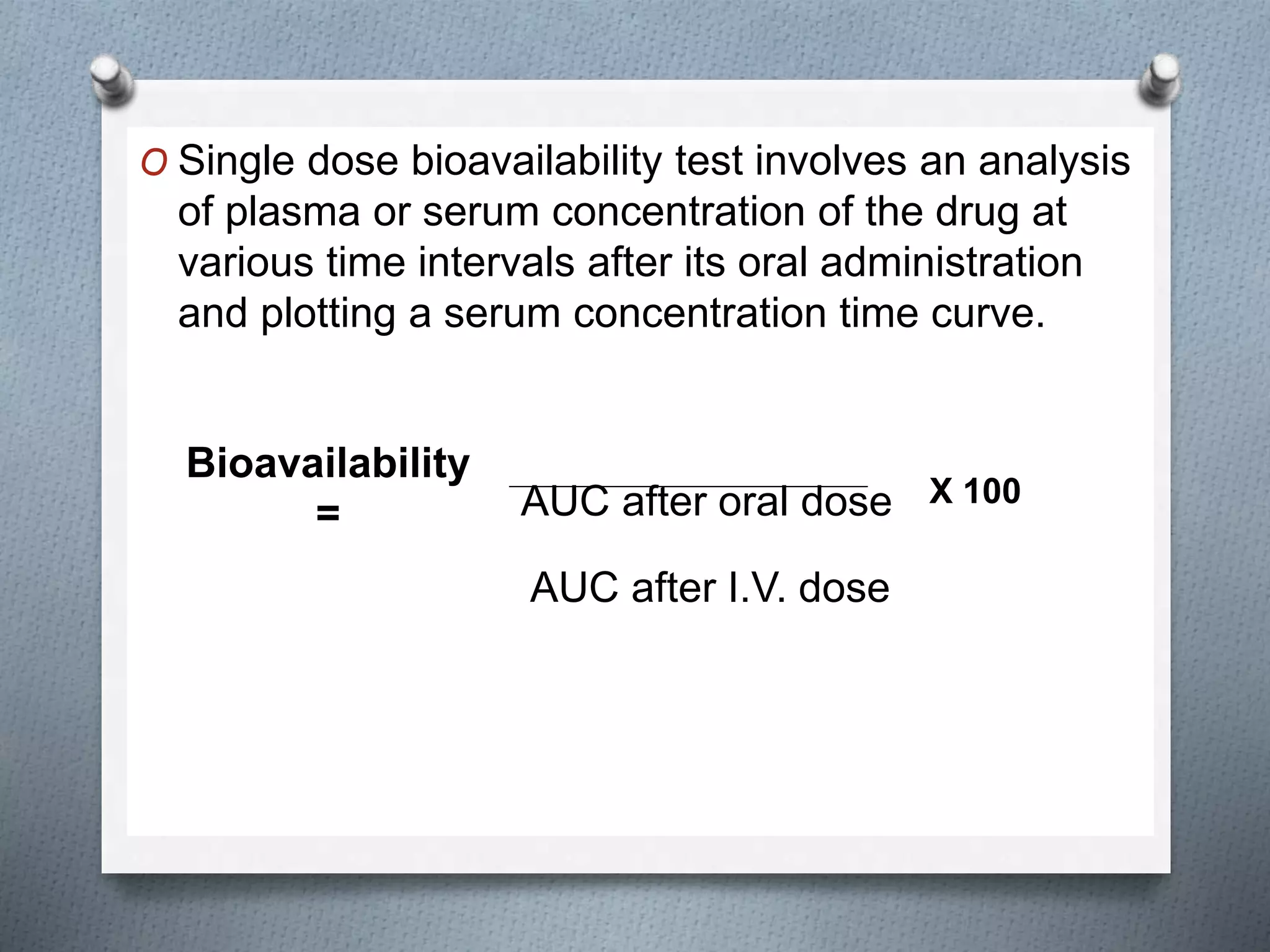






















This document provides an overview of pharmacokinetics, detailing the processes of drug absorption, distribution, metabolism, and excretion (ADME). It explains how drugs must be effectively administered and absorbed to reach their site of action, and the various factors that can influence these processes. Additionally, it covers concepts such as first-pass metabolism, drug bioavailability, and the impact of physiological and pharmaceutical factors on drug absorption.























































































