Downloaded 83 times

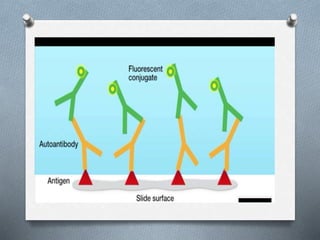




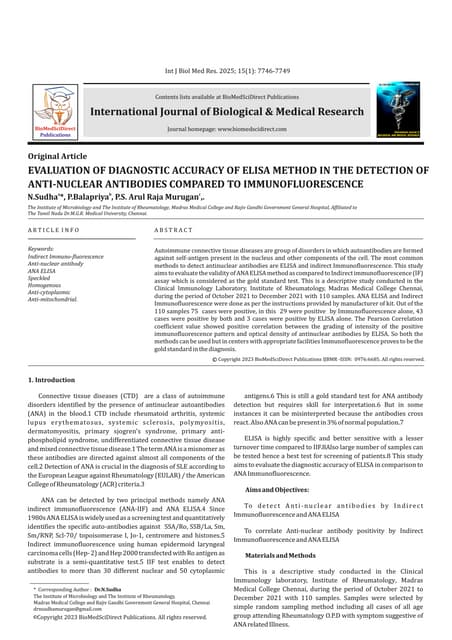
This document discusses autoantibodies and methods for detecting anti-nuclear antibodies (ANA). ANAs are antibodies directed against nuclear and cytoplasmic antigens and are associated with various autoimmune diseases. The three main methods for detecting ANAs are indirect immunofluorescence assay using HEp-2 cells, ELISA, and multiplex bead immunoassays. The immunofluorescence assay is commonly used for initial screening due to its ability to detect multiple antigen patterns but has limitations. ELISA and bead assays allow detection of specific autoantibodies and have improved sensitivity and specificity compared to immunofluorescence.























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















