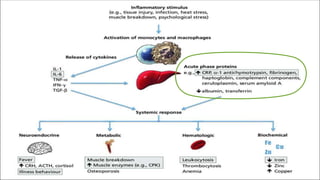
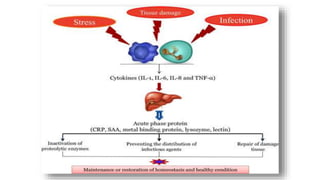
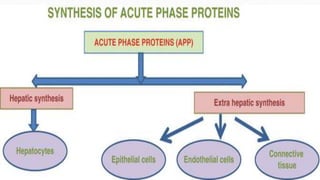
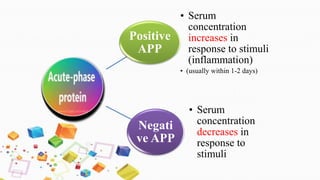
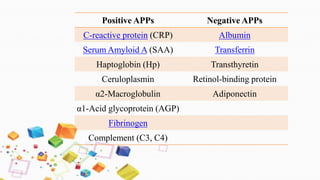
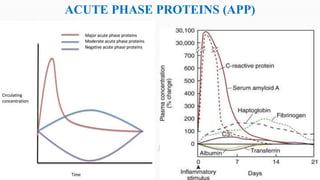
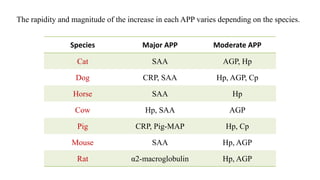
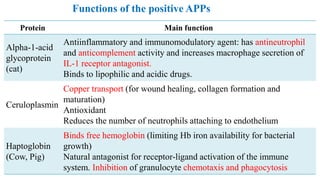
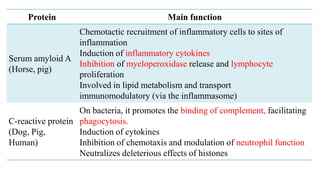
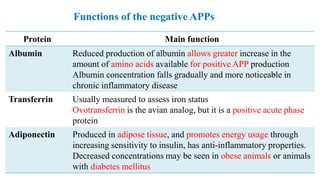
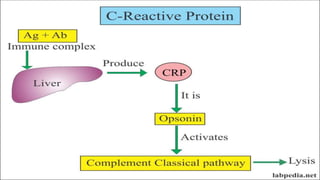
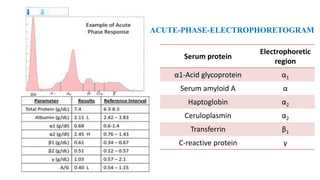
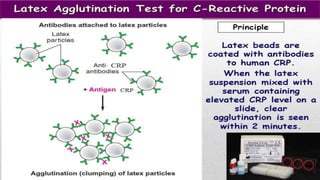
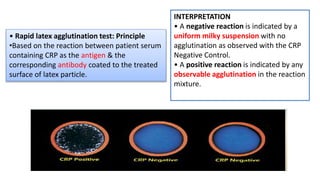
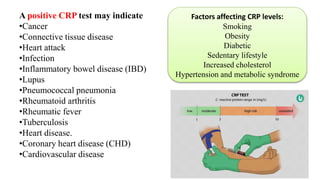
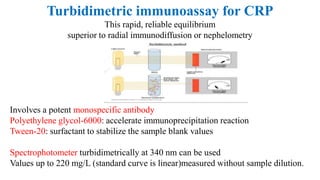
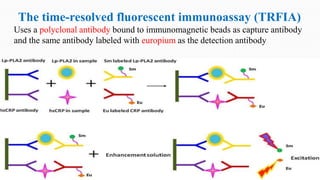
The document discusses acute phase proteins (APPs), which are proteins whose plasma concentrations increase or decrease in response to inflammation. It defines positive and negative APPs, provides examples of major, moderate, and minor APPs for different species, and describes the functions of key APPs like C-reactive protein (CRP), serum amyloid A, haptoglobin, ceruloplasmin, and alpha-1-acid glycoprotein. It also discusses methods for measuring APPs, including immunoassays, electrophoresis, and clinical importance of APPs like CRP.