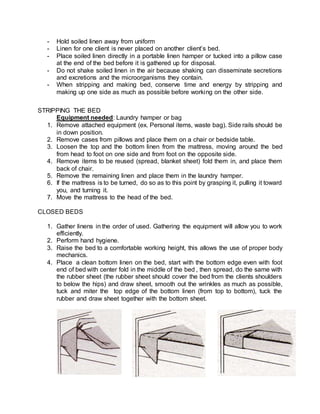
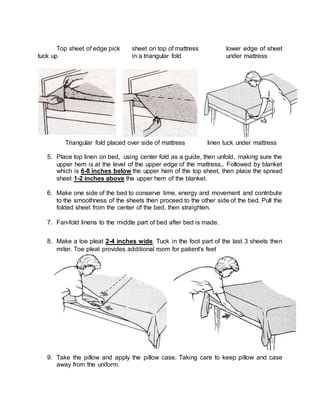
This document defines different types of bed making including open bed, occupied bed, surgical/post-op bed, and closed bed. It describes the purposes of bed making, components of hospital beds, commonly used bed positions, equipment needed for bed making, asepsis, body mechanics, guidelines, and steps for stripping beds and making open, closed, occupied, and post-op beds. The key information provided includes definitions of different bed types, purposes of providing a suitable environment and comfort for patients, common bed components, positions, necessary equipment, importance of asepsis, body mechanics, and specific steps for each bed making process.