Downloaded 36 times
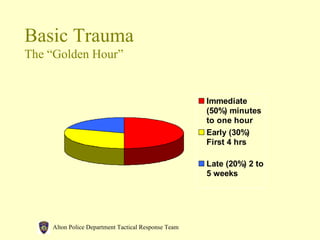





The document provides guidelines for rapid assessment and basic medical care during tactical operations to enhance injury survivability. It outlines systematic steps for assessing life-threatening injuries, emphasizes the importance of proper equipment and techniques, and details various first aid procedures for specific types of trauma. Key elements include a standard medical pouch content list and the necessity of spinal immobilization and communication with medical support during emergencies.









![Emergency Care[1]](https://cdn.slidesharecdn.com/ss_thumbnails/emergencycare1-090925233915-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)













































































