Downloaded 572 times
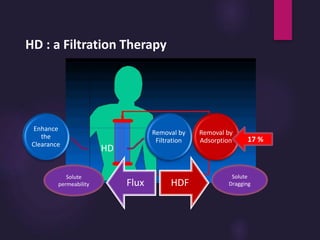
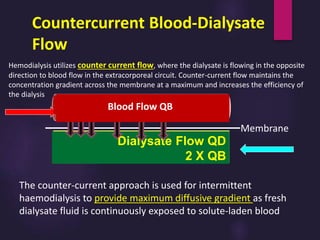
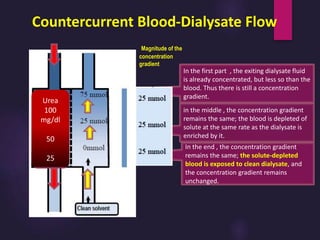
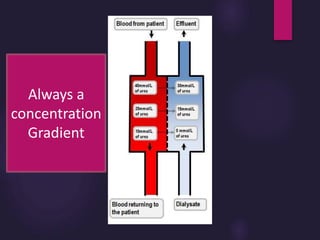
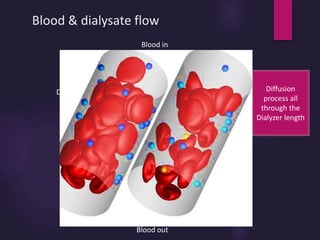
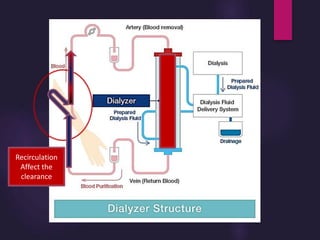
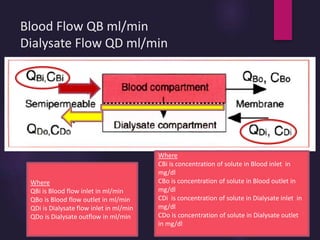
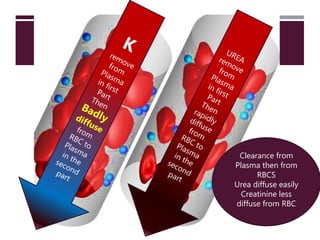
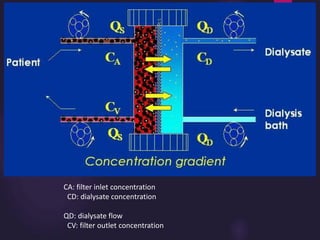
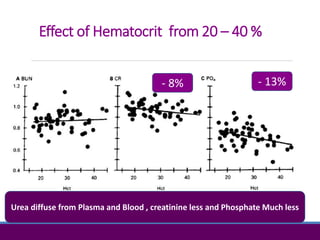
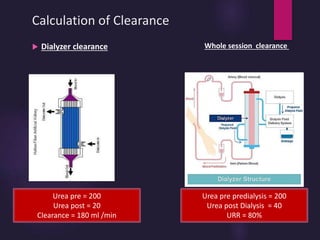
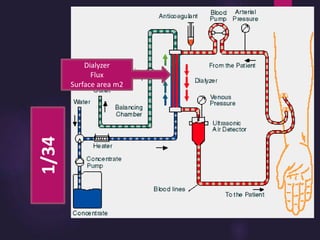
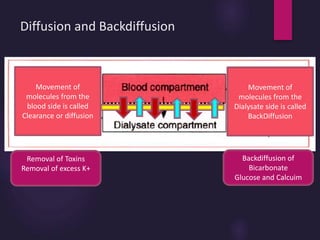
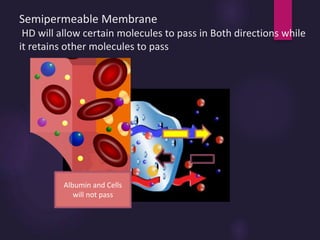
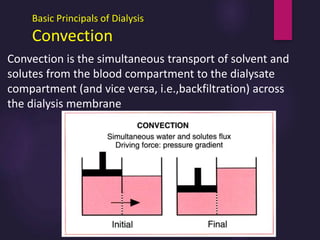
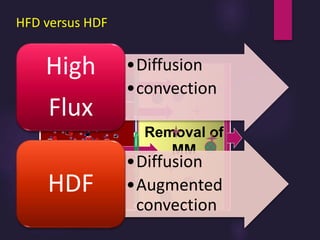
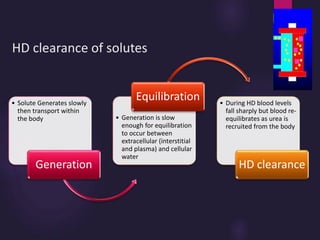
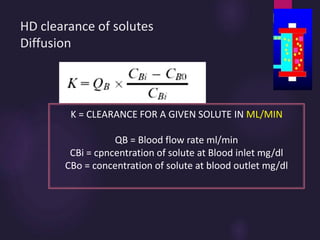
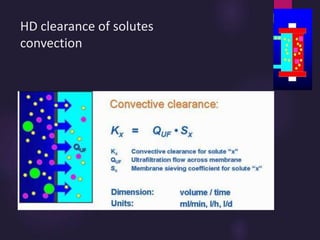
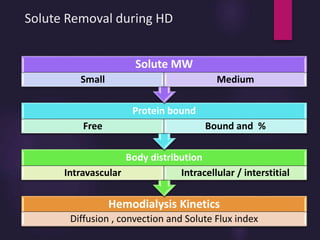
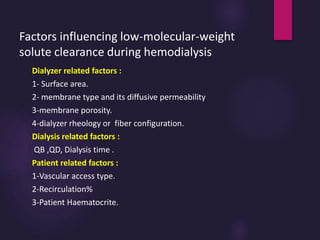
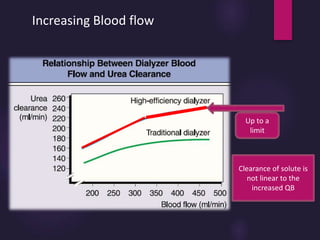
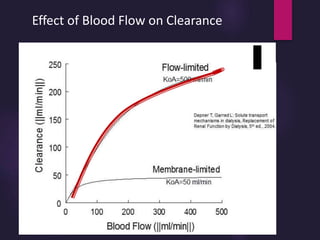
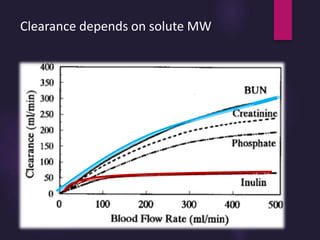
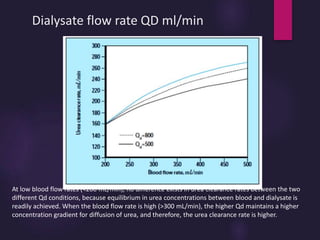
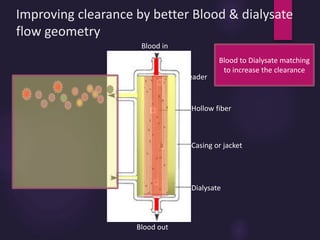

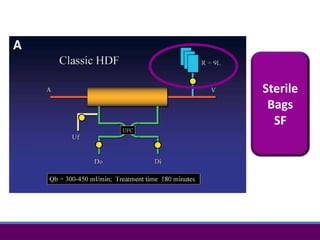
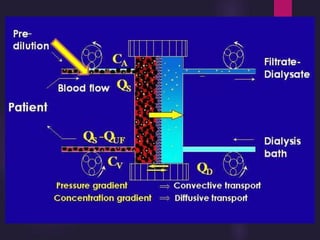
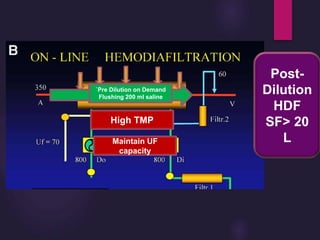
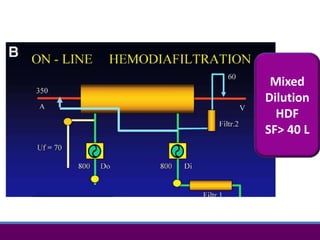

This document discusses the basic principles of hemodialysis. It covers: 1) Hemodialysis aims to remove waste, correct electrolytes, and remove excess fluids via diffusion, convection, and ultrafiltration across a semi-permeable membrane. 2) Countercurrent blood-dialysate flow maintains the concentration gradient to increase solute removal efficiency. 3) Clearance depends on factors like molecular weight, blood/dialysate flow rates, and dialyzer properties. Higher blood flows and matching dialysate flows can improve clearance.























































































