Normal Renal Functions
•Maintenance of body fluid composition
– volume, osmolality, electrolyte, acid-base regulations
• Excretion of metabolic end products and foreign substances (e.g.
medications)
• Neurohormonal
– renin, angiotensin, erythropoietin, 1,25-OH vitamin D
3.
The Dysfunctional Kidney
•Abnormal body fluid composition
– Fluid overload, sodium retention, hyperK+
, hyperphosphatemia,
acidosis
• Impaired excretion of substances
– Azotemia, uremia, intoxication or overdose
• Neurohormonal deficiencies or excess
– Hypertension, anemia, vitamin D deficiency, hyperparathyroidism
4.
Renal Replacement Therapy
•Therapy which replaces some or most of the functions of the
normal kidney
• Water handling: fluid removal
• Solute clearance: electrolytes, acids, metabolic byproducts, foreign
substances
• Water handling = ultrafiltration
• Solute clearance = dialysis
• Utilizes semipermeable membrane
IndicationstostartandstopRRT
• There isno consensus as to indication for initiation of RRT
• Common indications are azotemia, anuria, and complications of
AKI including pulmonary edema, severe fluid overload,
hyperkalemia and uncontrolled metabolic acidosis.
• Routine clinical practice is to adequately control fluid balance
and to a maintain a serum urea <30mg/dl, creatinine <2mg/dl
and normal electrolyte values.
7.
IndicationsforRRT
• Anuria –Oliguria (<200ml in 12hrs)
• Severe metabolic acidosis ( pH<7.10)
• Hyperazotemia ( BUN>80mg/dl) or creatinine > 4mg/dl
• Hyperkalemia K>6.5mEq/l
• Clinical signs of uremic toxicity
• Severe dysnatremia Na <115 or Na>160mEq/l
• Hyperthemia (>40 deg.C without response to medical therapy)
• Anasarca or severe fluid overload
• Multiple organ failure with renal dysfunction, sepsis or septic
shock with renal dysfunction
8.
Technique and modalities
•All RRTs consist of blood purification by having the blood flow
through a semi-permeable membrane
• Blood flow into hollow fibres composed by porous bicompatible
synthetic materials
• Wide range of substances ( water, urea and low, middle and high
MW solutes) leave the blood across such membranes by
diffusion( solutes) and by convection ( water and solutes)
9.
HEMODIALYSIS
Principles and TransportProcesses
• Dialysis is a process that facilitates the removal of excess water and
toxins from the body, both of which accumulate as a result of
inadequate kidney function.
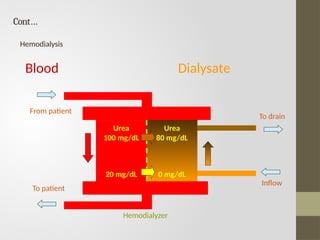
• DuringHD, a patient’s anticoagulated blood (circulated to the dialyzer
from a vein in the arm) and an electrolyte solution that simulates
plasma (dialysate) are simultaneously perfused through a dialyzer
(artificial kidney) on opposite sides of a semipermeable membrane.
• Solutes (e.g., metabolic waste products, toxins, potassium, and other
electrolytes) are removed from the patient’s blood by diffusing across
concentration gradients into the dialysate.
10.
Factorsaffectingrateofremoval
• Blood anddialysate flow rates through the dialyzer,
• Relative concentration of each solute in the blood and dialysis
solution (concentration gradients )
• Physical characteristics of the dialysis membrane (e.g., total
available surface area, thickness, and pore size)
• Properties (e.g., molecular size in daltons, molecular weight,
volume of distribution, and protein binding) of the solute being
removed.
NB: Because blood and dialysate flow in opposite directions
through the dialyzer, the concentration gradient for each solute
across the membrane is amplified
11.
Blood Dialysate
Urea
100 mg/dL
20mg/dL
Urea
80 mg/dL
0 mg/dL
Cont…
From patient
To patient
To drain
Inflow
Hemodialyzer
Hemodialysis
12.
ParticleMovement
Solutes from theblood are removed through diffusion and convection.
Diffusion is the process whereby the molecule moves across its
concentration gradient by passing through pores in the dialysis
membrane.
Once the concentration of a solute reaches equilibrium on both sides of
the membrane, the net movement is zero because the rate of movement
from the blood to dialysate compartment is equal to the rate from the
dialysate to the blood compartment. For most substances, equilibrium is
not achieved, either because the blood and dialysate flow rates are too
rapid, or the molecule is too large to easily move through the pores.
Convection is the process that removes toxins during dialysis through the
ultrafiltration of plasma water from the blood compartment. Controlled
pressure difference across the semipermeable membrane permits water
movement through the membrane pores, which carries with it solute into
the dialysate, thereby further enhancing solute removal. The removal of
solutes by convection during ultrafiltration generally is small relative to
their elimination through diffusion.
13.
DialyzerCharacteristics
• Dialyzers arecharacterized by many factors, such as membrane
composition, size, and ability to clear solutes
• Their primary component is the dialysis membrane, made of
cellulose
• Membranes differ not only by composition, but also by surface
area, thickness, and configuration within the dialyzer
• Functionally, dialysis filters can be differentiated based on their
ability to remove solutes and water
• Dialyzers are characterized as low-flux or high-flux based on pore
size and ability to remove small versus large molecules.
14.
BloodandDialysateFlow
• Although small-moleculeclearance is highly dependent on blood
flow, the relationship is not strictly linear.
• Increased blood flow yields a less than proportional response in
urea clearance. This is likely because of an insufficient time for
equilibration to occur between the blood and dialysate
compartments as well as a greater membrane resistance to
diffusion from an increased stagnant layer.
• A typical blood flow rate for dialysis is 400 to 500 mL/minute but
is dependent on the vascular access site and the cardiovascular
status of the patient.
• Some patients are not able to tolerate this rate, and a lower
blood flow rate may be necessary.
• Dialysate flow rates generally are 500 mL/minute and can be
increased to 800 mL/minute for high-flux dialysis,which will
increase urea clearance by approximately 10%.
15.
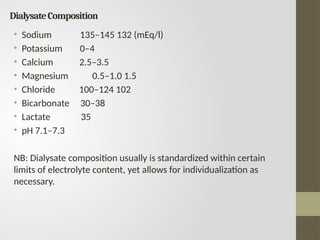
DialysateComposition
• Sodium 135–145132 (mEq/l)
• Potassium 0–4
• Calcium 2.5–3.5
• Magnesium 0.5–1.0 1.5
• Chloride 100–124 102
• Bicarbonate 30–38
• Lactate 35
• pH 7.1–7.3
NB: Dialysate composition usually is standardized within certain
limits of electrolyte content, yet allows for individualization as
necessary.
16.
VascularAccess
A permanent vascularaccess site provides easy access to high blood
flow, which cannot be achieved through routine venipuncture of
superficial veins.
Different types of vascular access are available:
• Arteriovenous (AV) fistula
• AV graft
• Central catheters
AV fistulas and grafts are placed in the nondominant arm. Ideal vascular
access delivers blood flow rates necessary for chronic HD, has a long
period of use, and has a low rate of complications (e.g.,. infection,
stenosis, thrombosis, aneurysm, and limb ischemia).
An AV fistula is preferred because of its longer survival of approximately
75% at 3 years (compared with 30% for the AV graft) and low rates of
complications.32
An AV fistula is created surgically by subcutaneous anastomosis of an
artery to an adjacent vein. During the dialysis procedure, one needle or
catheter is placed into the fistula site to deliver blood to the dialyzer.
17.
Cont…
Central venous cathetersare discouraged for chronic vascular access.
Although preferred, the AV fistula may not be suitable for patients with
poor vasculature, such as elderly patients or those with diabetes,
atherosclerosis, or small vessels.
The fistula should preferably be created 3 to 4 months before its
intended use to allow the vein to mature.
The graft can be used soon after insertion, although 2 weeks will allow
for healing at the anastomosis sites and may prolong patency.
Vascular access is critical for chronic HD and often has been labeled the
“Achilles’ heel” of dialysis therapy. Complications associated with
vascular access are a significant problem in patients having chronic HD.
The most common is thrombosis, usually the result of venous stenosis. If
not treated, thromboses will result in loss of the access
18.
Cont…
Access-related complications area major cause of hospitalization
and, therefore, attention to these problems is important clinically
and economically.
19.
Anticoagulation
Most patients havingHD are anticoagulated with IV heparin during the
dialysis treatment.
Anticoagulation is necessary to prevent blood from clotting in the
extracorporeal circuit for patients havingHD.
Several methods have been used in an attempt to provide adequate
anticoagulation without increasing the risk of bleeding.
Approaches include the administration of heparin in adequate quantities to
anticoagulate the patient during the dialysis procedure either by
intermittent bolus injections or an initial bolus followed by a continuous
infusion.
Modern HD delivery systems have incorporated heparin infusion devices
that can be programmed to provide the desired infusion rate during dialysis.
Another class of agents with potential use in patients requiring
anticoagulation during HD are the direct thrombin inhibitors, argatroban
and lepirudin (Refludan).
Their use is especially attractive in individuals who experience heparin-
induced thrombocytopenia (HIT).
FluidRemoval
• In additionto solute removal, the artificial kidney must be used to maintain
fluid balance in the patient without renal function.
• Most patients will become anuric once stabilized on HD, requiring control of
ingested fluids between treatment sessions.
• Fluid removal during dialysis then is necessary to achieve the “dry weight,” or
weight below which the patient could become symptomatic from volume
depletion.
• Achieving the dry weight is accomplished by ultrafiltration, through adjustment
of the transmembrane pressure.
• Negative pressure on the dialysate side of the membrane results in movement
of fluid across the membrane from the blood compartment.
• Dialysate membranes are characterized by their water permeability, or Kuf.
• Adjustment of the transmembrane pressure will provide the desired
ultrafiltration rate, based on the amount of fluid to be removed (predialysis
weight + IV saline + ingested fluids during dialysis – dry weight).
• For patients undergoing dialysis three times weekly, weight gains of 1 to 5 kg
are common between sessions.
• Modern hemodialyzers have built-in functions to adjust the transmembrane
pressure and remove fluid at a predetermined rate.
22.
Complications
1. Hypotension
• Thereported incidence of hypotension is10%to 30%, and even
higher in patients with specific risk factors, such as autonomic
dysfunction with diabetes and cardiac disease
• It is primarily caused by excessive fluid removal from the vascular
compartment at a rate exceeding mobilization of fluid stores
• Several pharmacologic agents have been proposed for the
management of hypotension, including
ephedrine,fludrocortisone, caffeine, vasopressin, L-carnitine,
sertraline, and midodrine.
23.
2. MuscleCramps
• Maybe induced by excessive ultrafiltration resulting in altered
perfusion of the affected tissues
• Several treatments have been attempted, including reduced
ultrafiltration and infusion of hypertonic saline or glucose to
improve circulation
• Exercise and stretching of the affected limbs also may be beneficial
• Long-term therapy may be directed at prevention with the use of
vitamin E 400 IU at bedtime.
• Vitamin E in combination with vitamin C 250 mg daily has been
found to be more effective than either therapy alone
24.
3.Hypersensitivity
• Reports ofanaphylactic reactions to dialyzer membranes, particularly
on initial exposure, may be directly related to the membrane itself, or
to ethylene oxide,which is commonly used to sterilize the dialyzer.
• Membranes most commonly responsible for reactions are
unsubstituted cellulose membranes (bioincompatible) or the high-flux
polyacrylonitrile membrane when used in conjunction with
angiotensin-converting enzyme (ACE) inhibitors.
• This latter reaction is thought to be related to the inhibition of
bradykinin metabolism by ACE inhibitors, resulting in an
anaphylactoid reaction.
25.
4. DialysisDisequilibrium
Dialysis disequilibriumis a syndrome that has been recognized since the
initiation of HD more than 30 years ago. Its etiology is related to
cerebral edema, and patients new to HD are at a greater risk because of
the accumulation of urea.
Rapid removal of urea from the extracellular space lowers the plasma
osmolality, thereby leading to a shift of free water into the brain.
Lowering of intracellular pH, as can occur during dialysis, has also been
suggested as a cause.
Clinical manifestations occur during or shortly after dialysis and include
central nervous system (CNS) effects, such as headache, nausea, altered
vision, and in some cases, seizures and coma.
Treatment is aimed at prevention by initiating dialysis gradually by using
shorter treatment times at lower blood flow rates in new patients.
Direct therapy can be provided in the form of IV hypertonic saline or
mannitol.
26.
5.Thrombosis
• Access lossis most often the result of thrombosis,which is usually
a consequence of venous stenosis
• The stenosis may be corrected by percutaneous transluminal
angioplasty (PCTA) or, if necessary, surgical revision of the access
site
• Successful correction is effective as a means to prevent
thrombosis
• Once it occurs, thrombosis is managed by surgical thrombectomy
or with pharmacomechanical or mechanical thrombolysis.
• Thrombolytic therapy, administered by pulse spray technique of
urokinase or streptokinase, combined with mechanical
thrombectomy is as effective as surgical thrombectomy.
27.
6.Infection
• Access infections,usually involving grafts to a greater extent than a
native fistula, are predominantly caused by Staphylococcus aureus or
S. epidermidis .
• Infections with gram-negative organisms as well as Enterococcus
occur with a lower frequency.
• Access infections can lead to bacteremia and sepsis with or without
local signs of infection.
• Treatment usually is initiated with vancomycin, administered as a
single, 1-g dose, repeated as necessary, depending on the type of
dialysis being used, or cefazolin 20 mg/kg three times weekly, and
gentamicin 2 mg/kg with appropriate serum concentration
monitoring.
• High-flux dialysis results in greater removal of vancomycin than
conventional dialysis and, therefore, more than a single dose may be
necessary for adequate treatment
PERITONEAL DIALYSIS
• Peritonealdialysis is performed using several different modalities,
including the most common, continuous ambulatory peritoneal
dialysis.
• Development of specialized devices to facilitate the exchange
process and improve patient convenience has led to processes
referred to as automated peritoneal dialysis, including continuous
cycling peritoneal dialysis (CCPD) and nocturnal intermittent
dialysis (NIPD)
• CAPD is the most common method for chronic PD, but the APD
methods are rapidly growing.
30.
PrinciplesandTransportProcesses
• Continuous ambulatoryperitoneal dialysis is performed by the instillation of
2 to 3 L of sterile dialysate solution into the peritoneal cavity through a
surgically placed resident catheter.
• The solution dwells within the cavity for 4 to 8 hours, and then is drained and
replaced with a fresh solution.
• This process of fill, dwell, and drain is performed three to four times during
the day, with an overnight dwell by the patient in his or her normal home or
work environment.
• Conceptually, the process is similar to HD in that uremic toxins are removed
by diffusion down a concentration gradient across a membrane into the
dialysate solution.
• In this case, the peritoneal membrane covering the abdominal contents
serves as an endogenous dialysis membrane, and the vasculature embedded
in the peritoneum serves as the blood supply to equilibrate with the
dialysate.
• A primary difference is that because the dialysate solution is resident, the
result is a very slow dialysate flow rate of approximately 7 mL/minute when
10 L of fluid is drained per day. Solute loss occurs by diffusion for small
molecules, and through convection for larger, middle molecules.
31.
BloodandDialysateFlow
• Hemodialysis providesconstant perfusion of fresh dialysate, thereby
maintaining a large concentration gradient across the dialysis
membrane throughout the dialysis treatment.
• During a typical dwell period for CAPD, urea and other substances
increase in the dialysate relative to unbound plasma concentrations.
• For a daytime dwell period of 4 hours, urea achieves nearly equal
concentrations with plasma; therefore, the rate of elimination can
become very small
• Instillation of fresh dialysate solution will re-establish the diffusion
gradient leading to an increased rate of urea removal. For a patient
making four exchanges of 2 L each per day, assuming the urea
dialysate concentration equals the plasma concentration, and 2L are
removed by ultrafiltration, the urea clearance would be
approximately 7 mL/minute. This is substantially lower than urea
clearances achieved with HD; therefore, CAPD must be performed
continually throughout the week to achieve adequate urea removal
32.
Cont…
• Clearance dependson blood flow; dialysate flow; and peritoneal membrane
characteristics, such as size, permeability, and thickness.
• Dialysate flow, the only easily adjusted variable to alter clearance, has been used
effectively in acute PD to achieve relatively high clearances with 30- to 60-minute dwell
periods in a cycling system.
• CCPD uses this concept of shorter dwell periods during the sleeping hours with
automatic fill, dwell, and drain periods, leaving a high-dextrose dialysate in the
peritoneal cavity throughout the day until the next cycling session.
• NIPD is similar, with nightly exchanges, but the peritoneum is left unfilled, or dry, during
the daytime. As a result, urea clearance is lower with NIPD, but may be suitable for
many patients, and preferable to the volume load in the peritoneal cavity throughout
the day with CCPD.
• Electrolyte concentrations in the dialysate solution are near physiologic concentrations
to prevent substantial shifts in serum electrolyte levels.
• A potential advantage of PD compared with HD is the continuous dialysis of larger,
middle molecules that may exert toxic effects.
• These molecules are cleared through convection and follow water as it is removed
through ultrafiltration.
• Clearance of these molecules depends less on flow and more on duration of dialysis.
The continuous process of PD, albeit associated with low clearance values, provides for
a more physiologic condition in patients, rather than the intermittent treatment
provided with HD.
33.
FluidRemoval
• Fluid isremoved by ultrafiltration through adjustment of the
transmembrane pressure during HD.
• Because this pressure is not easily adjusted in PD, fluid is removed by
altering the osmotic pressure within the dialysate. This is accomplished
by the addition of dextrose monohydrate to the dialysate in varying
concentrations, depending on the degree of fluid removal necessary in
the patient.
• Concentrations of dextrose in commercially available solutions include
1.5%, 2.5%, and 4.25%, with net fluid losses during a 4-hour dwell period
of 200 and 400 mL for the 1.5% and 2.5% solutions, respectively, and
approximately 700 mL for the 4.25% solution following an overnight
dwell.
• As the dwell time persists, the dextrose is absorbed and is diluted by the
movement of fluid from the vascular space, so that most ultrafiltration
occurs early during the dwell period.
• Acid-base balance is achieved through the absorption of lactate from the
dialysate, which subsequently is metabolized to bicarbonate in vivo.
Bicarbonate is not compatible with the calcium and magnesium in the
dialysate and can lead to precipitation.
34.
Access
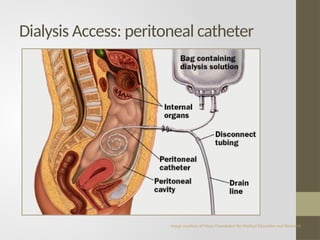
• Delivery ofdialysate into the peritoneal cavity is accomplished through an
indwelling catheter inserted through the abdominal wall.
• The most common design is the Tenckhoff catheter, made of silicone rubber
or polyurethane; it consists of a tube, straight or curled, with many holes in
the distal end for fluid inflow and Outflow.
• The catheter also has a single or double cuff, which serves to anchor it to
the internal and external attachment sites by promoting fibrous tissue
growth; this also serves as a barrier to bacterial migration.
• Several modifications to the original catheter have appeared on the market,
mostly in an attempt to overcome problems related to outflow of dialysate.
Maintaining an unobstructed outlet port is essential for successful PD.
• Delivery of dialysate through the catheter is accomplished in several
modes. A straight transfer set uses tubing attached to the catheter at one
end, and to the bag of dialysate at the other, via a spike.
• The transfer set usually is changed every 1 to 2 months in the dialysis clinic.
• For each dialysate exchange, the patient attaches a bag of fresh dialysate,
warmed to body temperature, to the transfer set and infuses the solution.
DialysisPrescription
• The initialCAPD prescription for most patients consists of three
exchanges during the day with 1.5% dextrose and a fourth, overnight
exchange with 4.25% dextrose.
• This would be expected to achieve fluid removal of approximately 1,300
mL, based on 200 mL from each daytime exchange and 700 mL
overnight.
• Based on assessment of the patient’s fluid status, it may be necessary
to increase or decrease the dialysate prescription to achieve fluid
balance.
• Fluid retention is solved by increasing the dextrose content of the
daytime exchanges, beginning with 2.5% in place of one of the 1.5%
solutions. This is expected to result in an additional removal of 200 mL,
and therapy can be further adjusted as necessary.
• For patients with excessive fluid removal, it may be possible to decrease
the number of exchanges per day as long as adequate solute removal is
present. If four exchanges are needed, the fluid intake can be liberalized
to maintain adequate hydration.
37.
Complications
Peritonitis
• The mostsignificant complication among patients having PD is peritonitis,which is
frequently caused by coagulase-negative staphylococci, including S. epidermidis
(30.6%) or S. aureus (17.5%).
• The patient usually presents with abdominal pain, nausea and vomiting, and fever
with or without a cloudy effluent.
Exit-Site Infection
• Prevention of catheter exit-site infections (and thus peritonitis) is the primary goal
of exit-site care.
• Several preventative measures are important: adequate catheter placement,
dedicated postoperative catheter care, and routine daily care of the exit site.
Weight Gain
• Approximately 500 to 1,000 kcal/day are absorbed as glucose from PD solutions,
which can lead to weight gain in patients.
• Some patients may require modification of oral caloric intake to avoid excessive
weight gain.
• Insulin requirements generally are increased in patients with diabetes as a result
of the additional calories