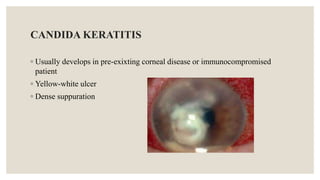
The document outlines infective corneal ulcers, detailing their definitions, types, etiologies, symptoms, diagnosis, and management principles. It emphasizes the distinction between infectious and non-infectious keratitis, highlighting the critical need for timely treatment to prevent vision loss. The management strategies include infection control, inflammation management, and re-epithelialization promotion, with specific treatments based on the underlying cause of the corneal ulcer.






























![DOC-20250918-WA0006^[1].pptx bhfhhfdhfhdy](https://cdn.slidesharecdn.com/ss_thumbnails/doc-20250918-wa00061-251230130620-d87c8ec0-thumbnail.jpg?width=640&height=640&fit=bounds)
























