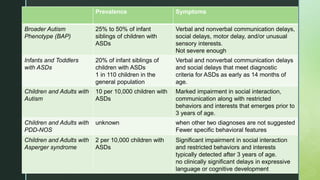
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition primarily affecting social interaction, communication, and behavior, with a marked predominance in males. The disorder's symptoms often present before age three and include significant deficits in social skills, communication, and the presence of repetitive behaviors, with varying severities categorized as autism, Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS), and Asperger syndrome. Although no single cause is identified, genetic and environmental factors play roles in its etiology, while early diagnosis and intervention are crucial for improving outcomes.