Downloaded 94 times













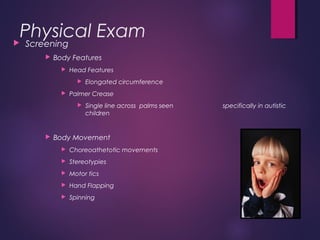
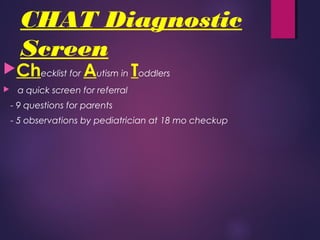
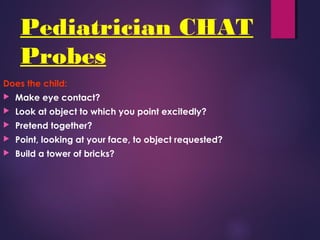
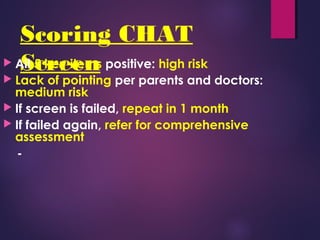




The document discusses the early diagnosis of autism spectrum disorder (ASD), outlining essential red flags for identifying the condition in children, including social, communication, and behavioral milestones. It emphasizes the importance of early intervention, noting that intensive behavioral modifications can significantly improve outcomes for those diagnosed early. Additionally, the document addresses misconceptions regarding treatment and highlights genetic factors associated with autism risk.