Downloaded 35 times













































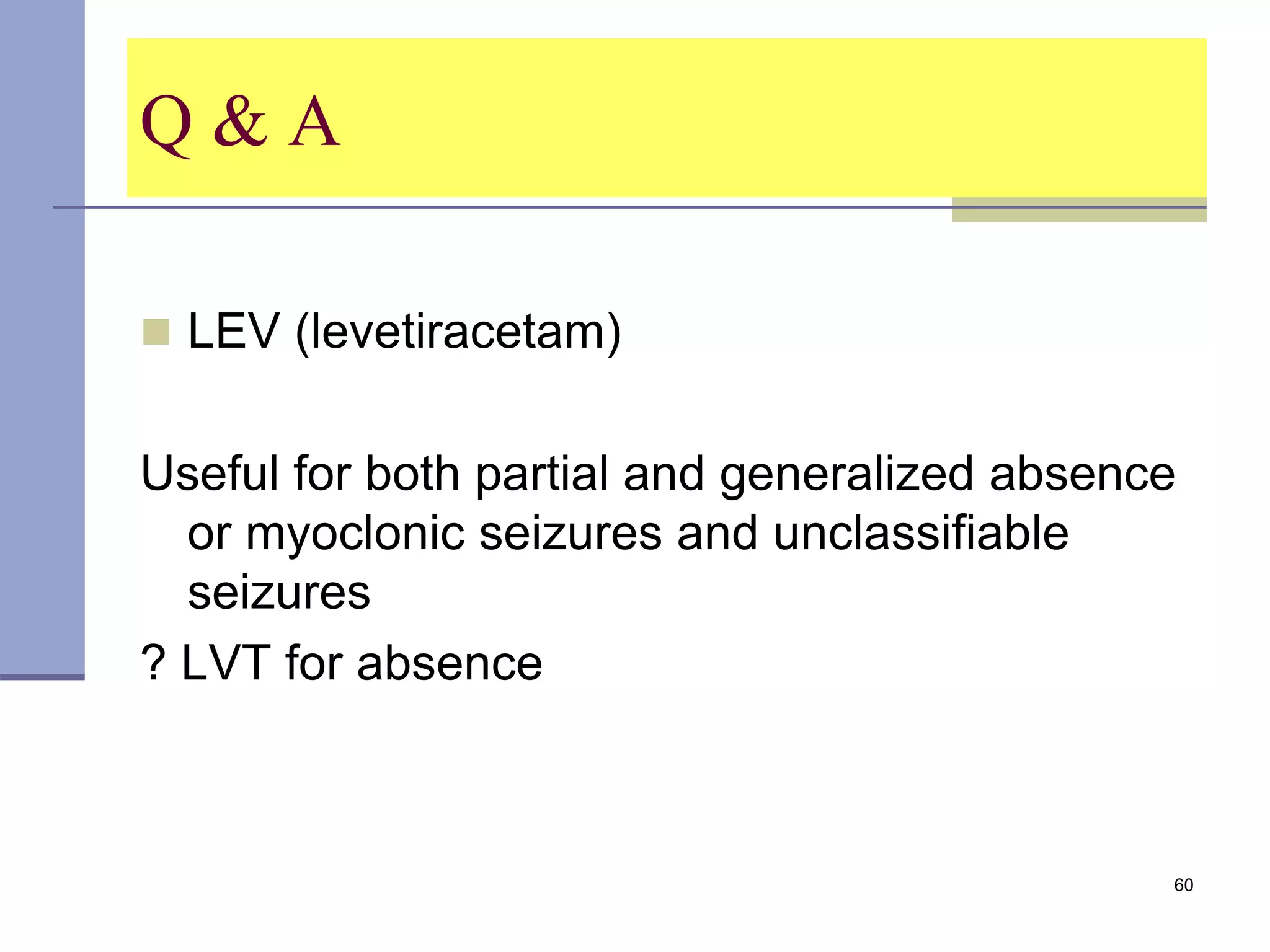






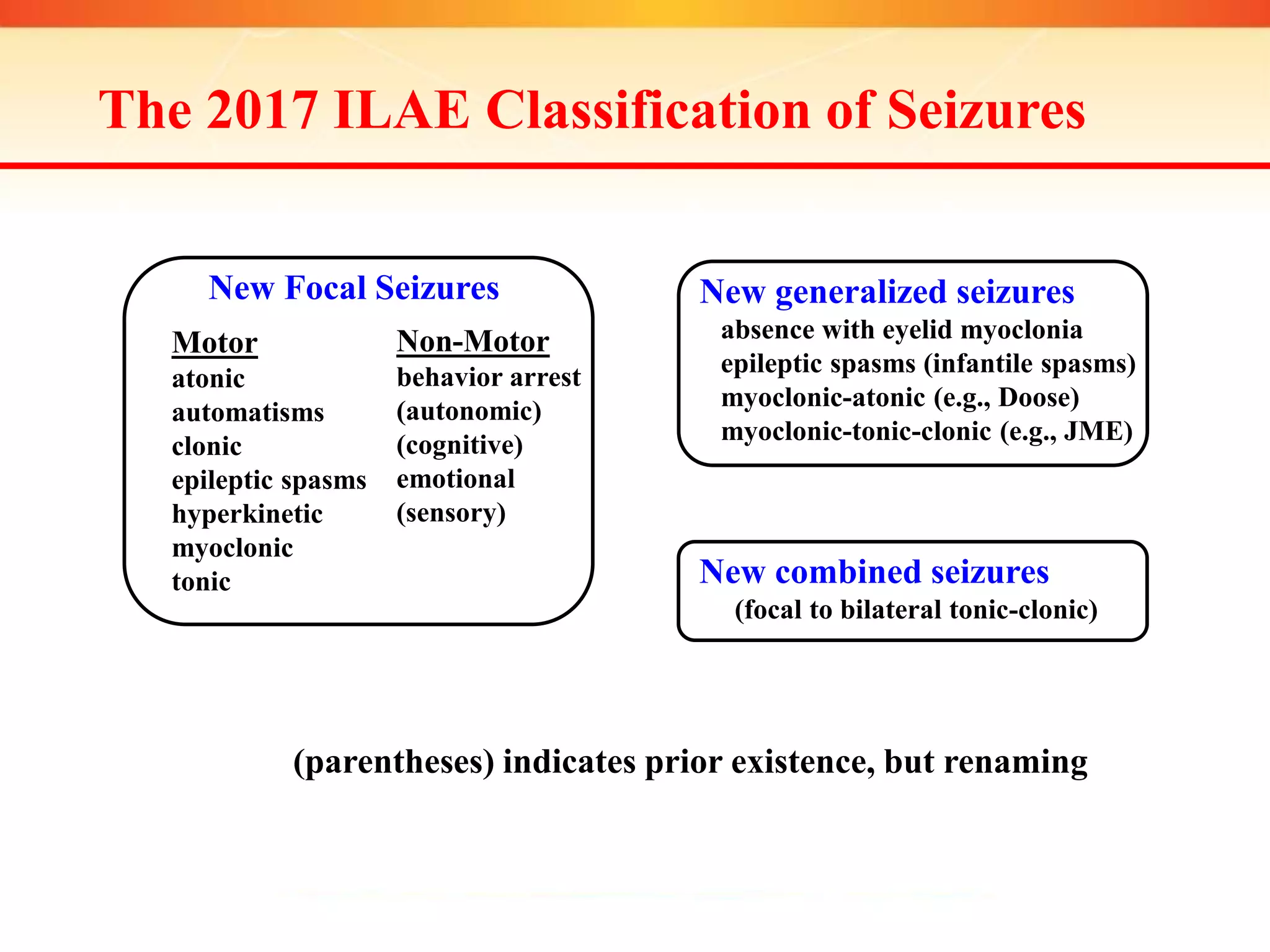


The document provides information on epilepsy classification, diagnosis, and treatment. It discusses: 1. The 2017 ILAE classification system for seizures, which categorizes seizures as focal or generalized based on onset and includes motor and non-motor seizure types. 2. Factors that can help diagnose epilepsy including EEG, MRI/CT scans, and seizure description/videos. An EEG is most valuable within 24 hours of a seizure. 3. Treatment considerations like using broad-spectrum anti-epileptic drugs (AEDs) like levetiracetam as first-line due to few drug interactions and cognitive side effects. AED treatment should begin after the first seizure in adults.























































































