Downloaded 55 times



This document provides information on G6PD deficiency and favism. It describes a case of a 3-year old boy presenting with pallor, red urine, and abdominal pain, which are signs of hemolytic anemia. It then discusses the characteristics of hemolytic anemia and explains that G6PD deficiency is a genetic disorder where individuals are at risk of hemolytic anemia when consuming fava beans or certain drugs due to inadequate NADPH production and antioxidant effects in red blood cells. The document concludes with treatment recommendations of blood transfusions and avoiding triggers like fava beans, certain medications, infections, and chemicals for people with G6PD deficiency.
Overview of G6PD deficiency and its significance for clinical pharmacy students, presented by Prof. Dr. Hussein Abdeldayem.
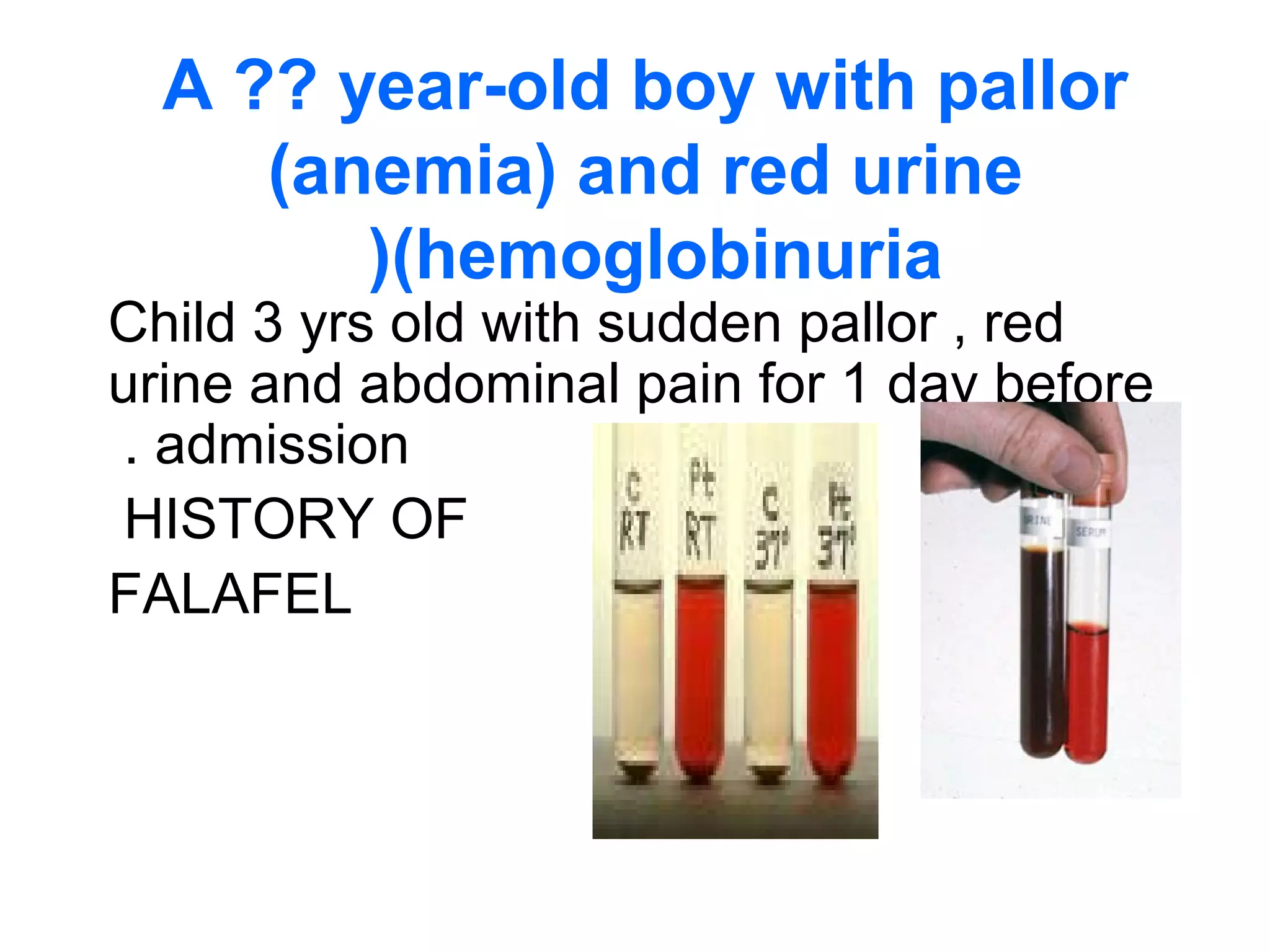
A 3-year-old boy with anemia and red urine, highlighting dietary history including falafel as a possible trigger.
Characteristics of hemolytic anemia include pallor, increased reticulocyte count, and hyperbilirubinemia.
G6PD deficiency is X-linked; variants affect populations differently. It's crucial for understanding patient risks.
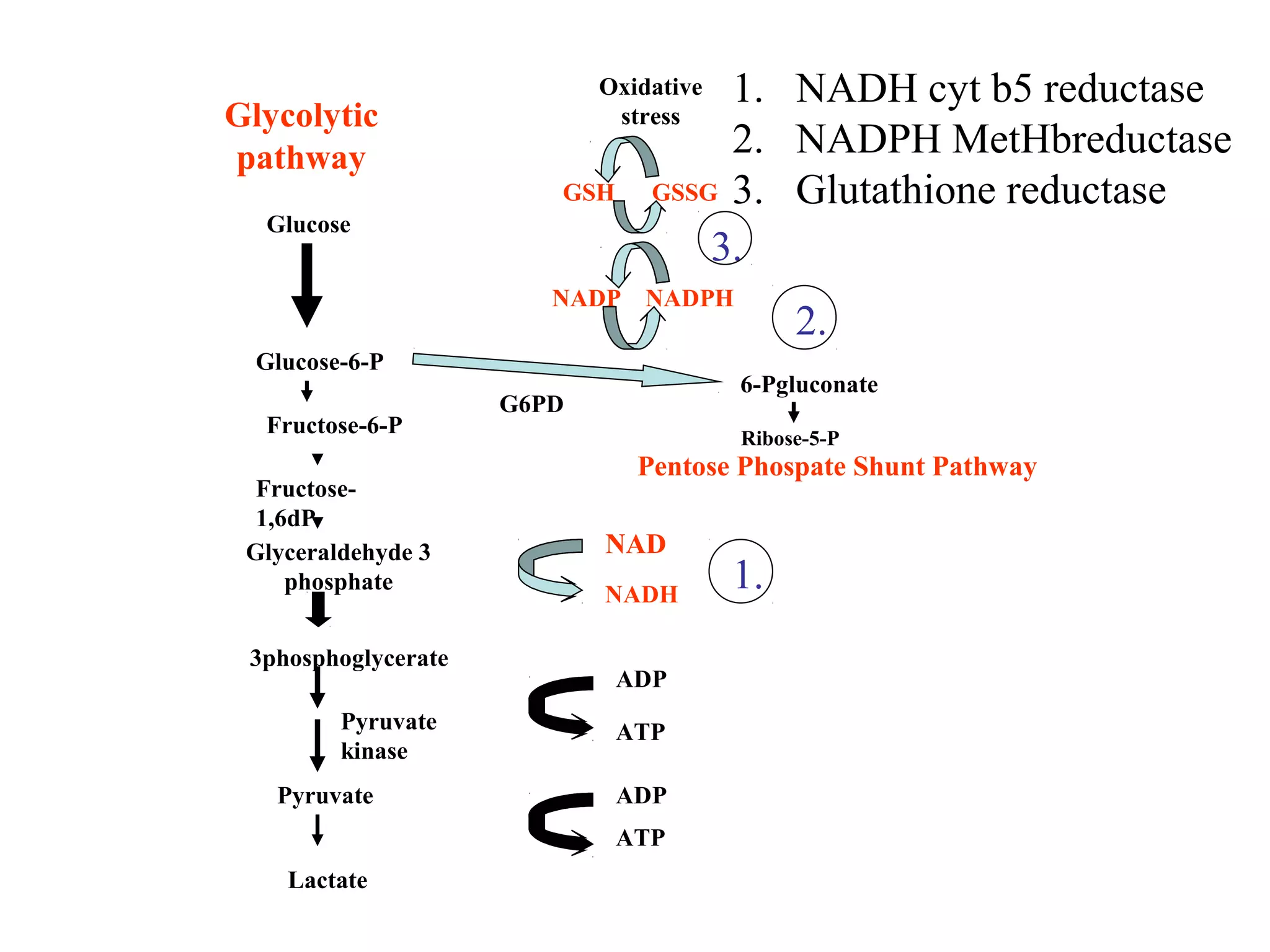
Overview of metabolic pathways and the role of G6PD in oxidative stress and red blood cell function.
Treatment involves hospitalization and packed RBC transfusion; emphasizes the need for G6PD enzyme assays.
Foods, drugs, and chemicals to avoid include fava beans and certain medications, stressing their dangers.