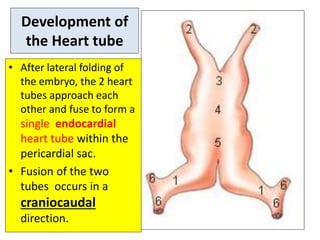
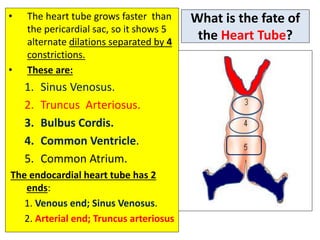
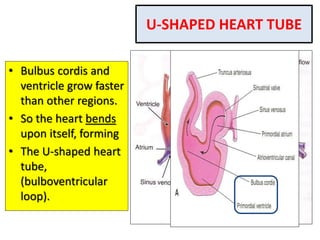
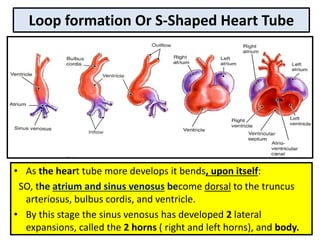
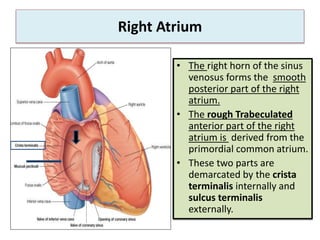
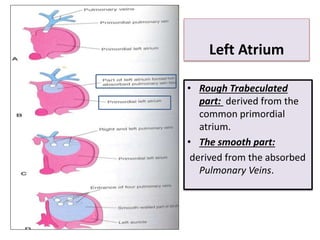
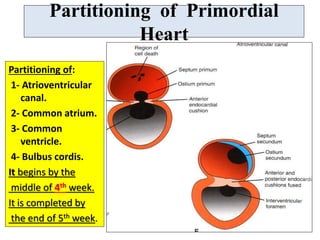
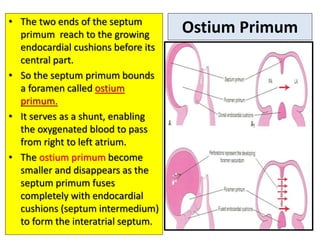
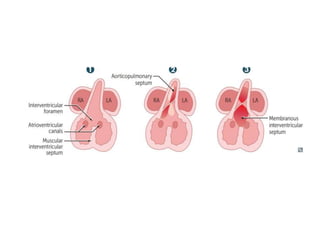
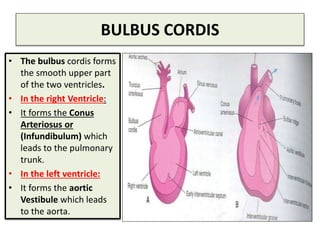
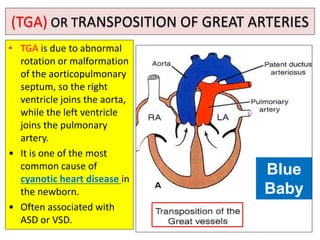
This document describes the development of the heart from a single heart tube to the four-chambered heart. It discusses how the heart tube partitions to form the atria and ventricles through formation of septa. The fate of the sinus venosus and bulbus cordis are also described. Finally, some common cardiac anomalies are listed such as atrial and ventricular septal defects, Tetralogy of Fallot, transposition of the great arteries, and persistent truncus arteriosus.