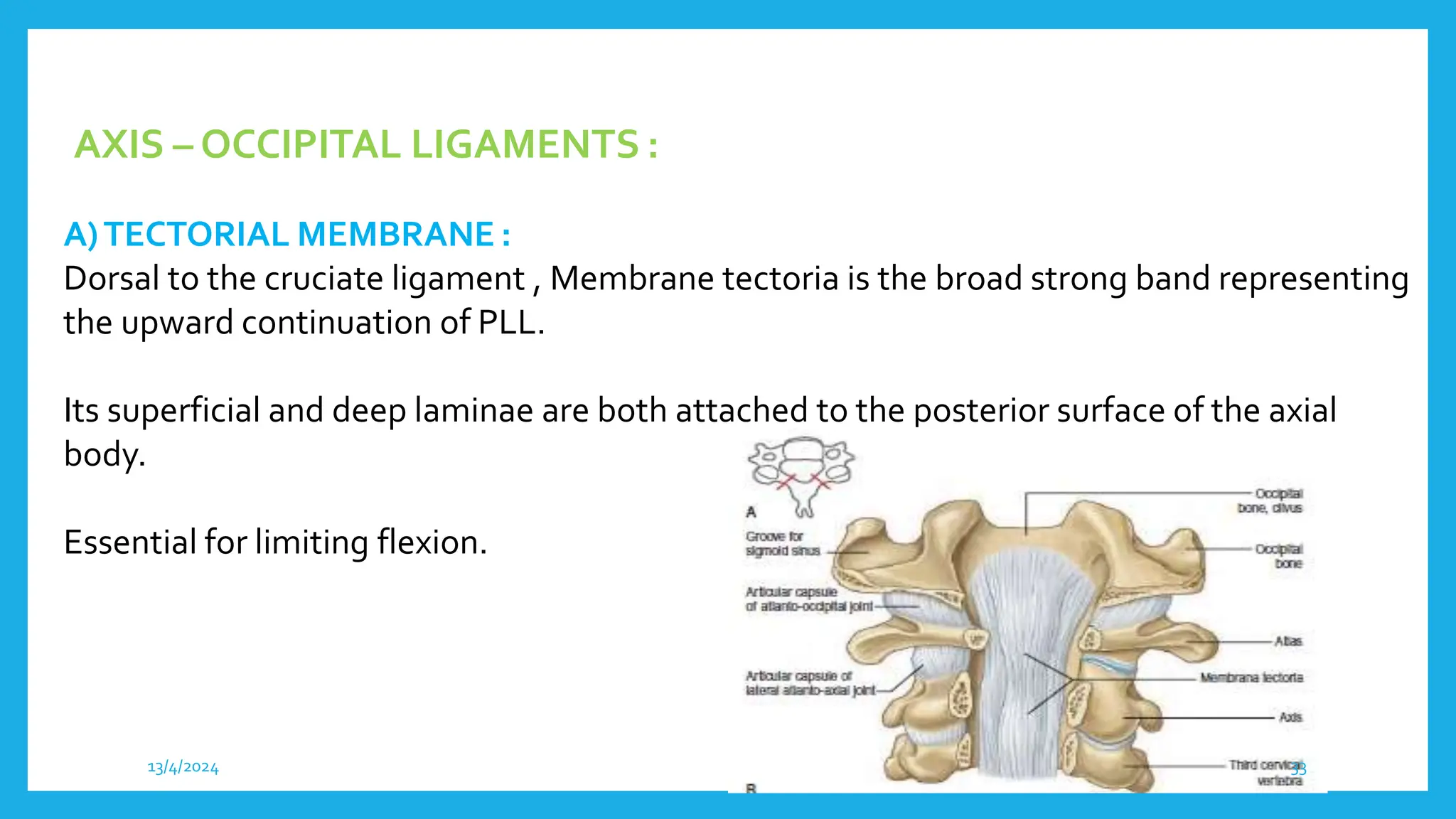
The craniovertebral junction (CVJ) refers to the occiput, atlas, axis, and supporting ligaments. It forms a transition zone between the mobile cranium and rigid spinal column, enclosing the cervicomedullary junction. The key components of the CVJ include the occipital bone, atlas, axis, occipitoatlantal and atlantoaxial joints, and stabilizing ligaments like the transverse atlantal ligament and alar ligaments. Radiological imaging like plain radiographs, CT, and MRI are useful for evaluating the bony and soft tissue anatomy of the CVJ and detecting any abnormalities.