

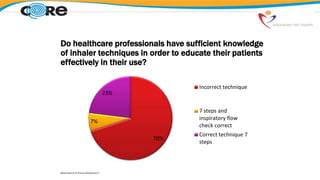
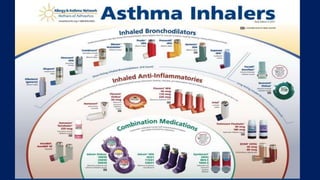
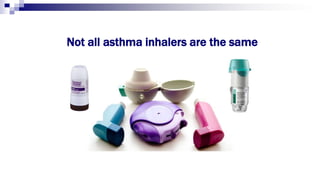
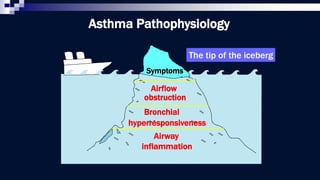
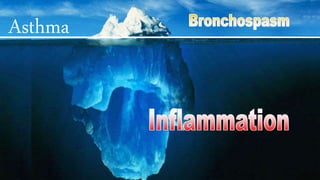



















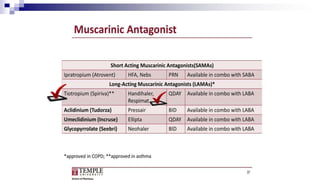


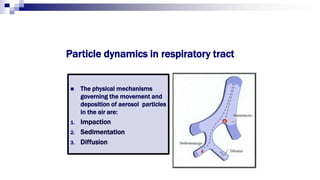
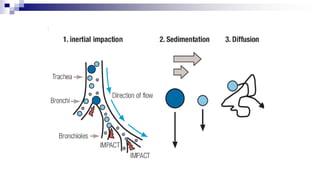
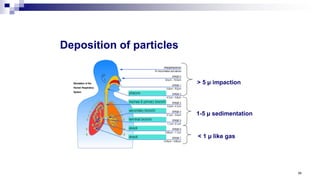
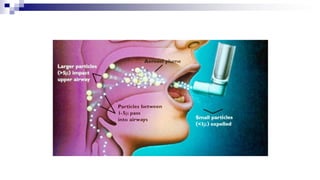
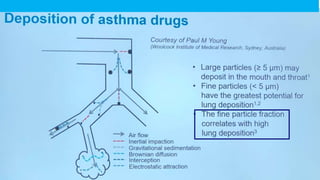
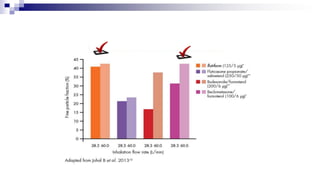
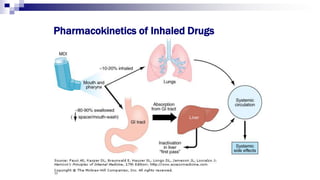
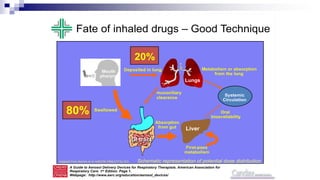
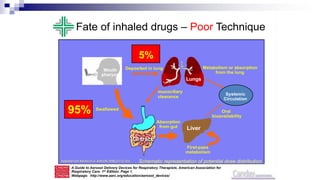




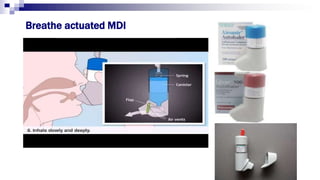












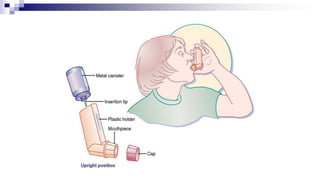
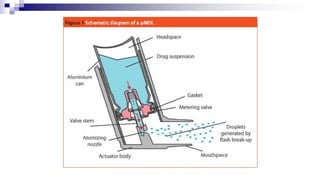



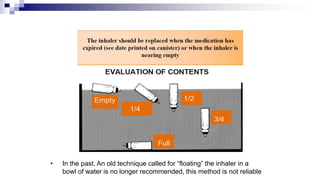

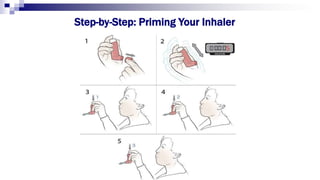
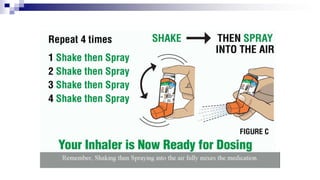
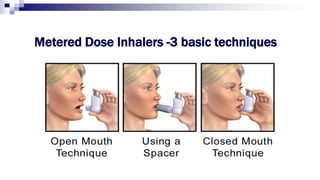
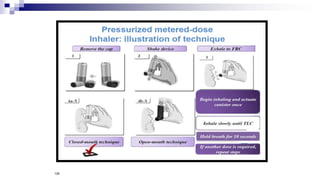
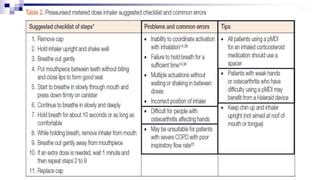




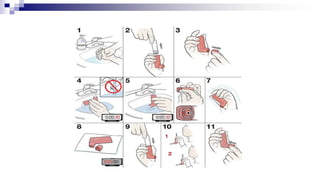















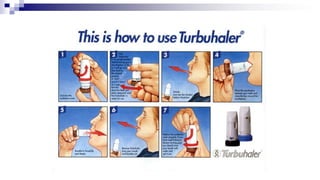
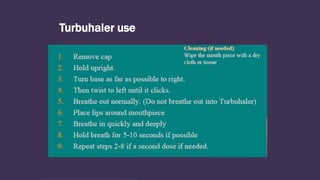



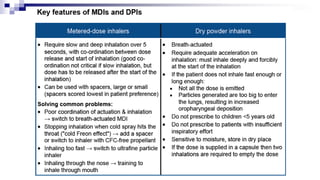










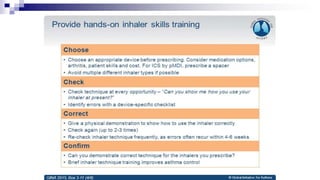
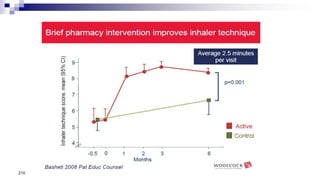



The document discusses reasons for poor asthma control and strategies for improving inhaler technique and medication adherence. Some key points include: - Poor asthma control can be due to incorrect diagnosis, improper inhaler technique, smoking, comorbid rhinitis, nonadherence to treatment, or inadequate treatment. - Healthcare providers need proper training to effectively educate patients on correct inhaler use. - Factors like particle size, inspiratory flow, and inhaler technique affect lung deposition and treatment effectiveness. - Common inhaler devices include pressurized metered dose inhalers, dry powder inhalers, and soft mist inhalers. Proper priming, shaking, exhal




















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


