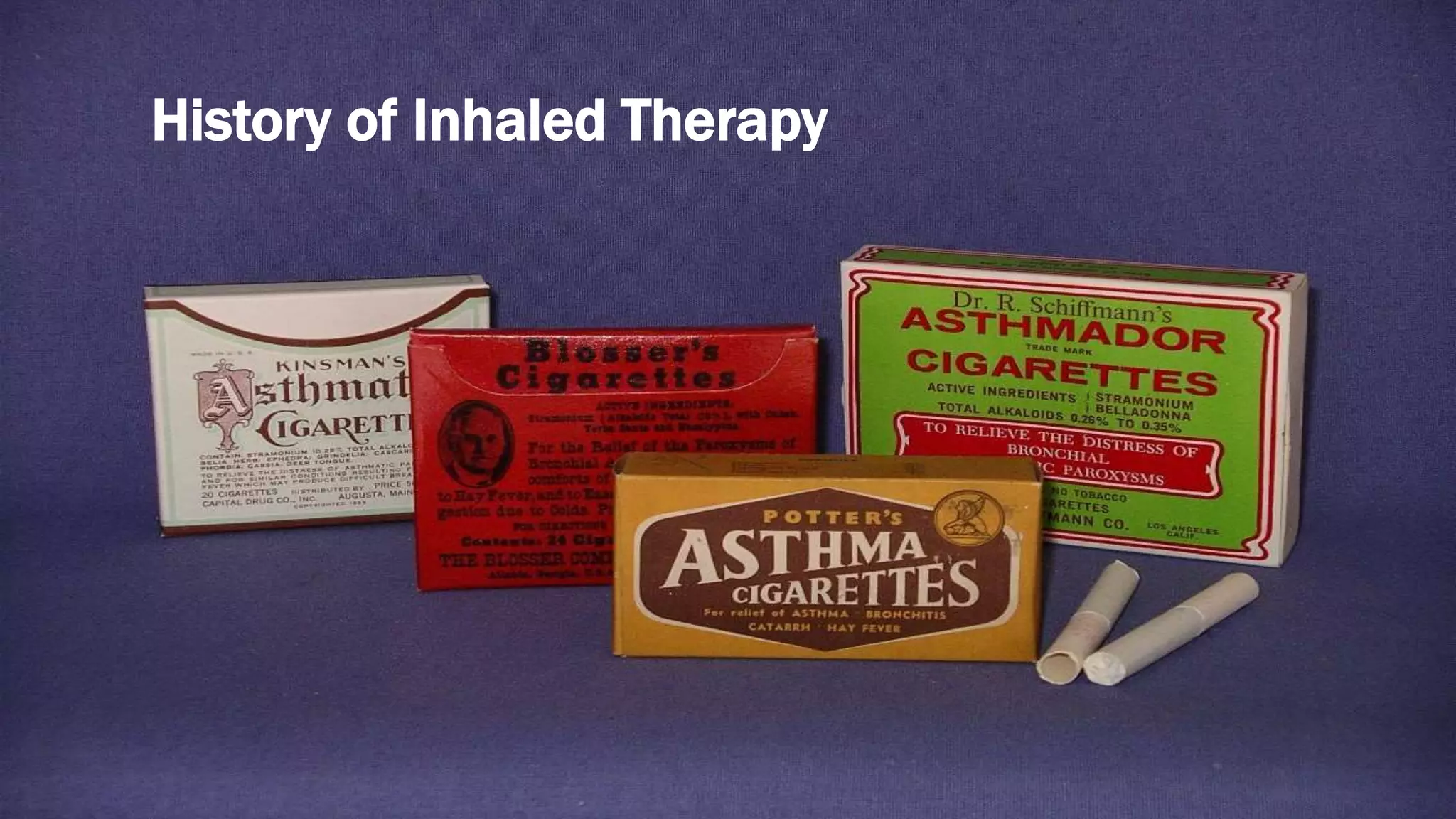
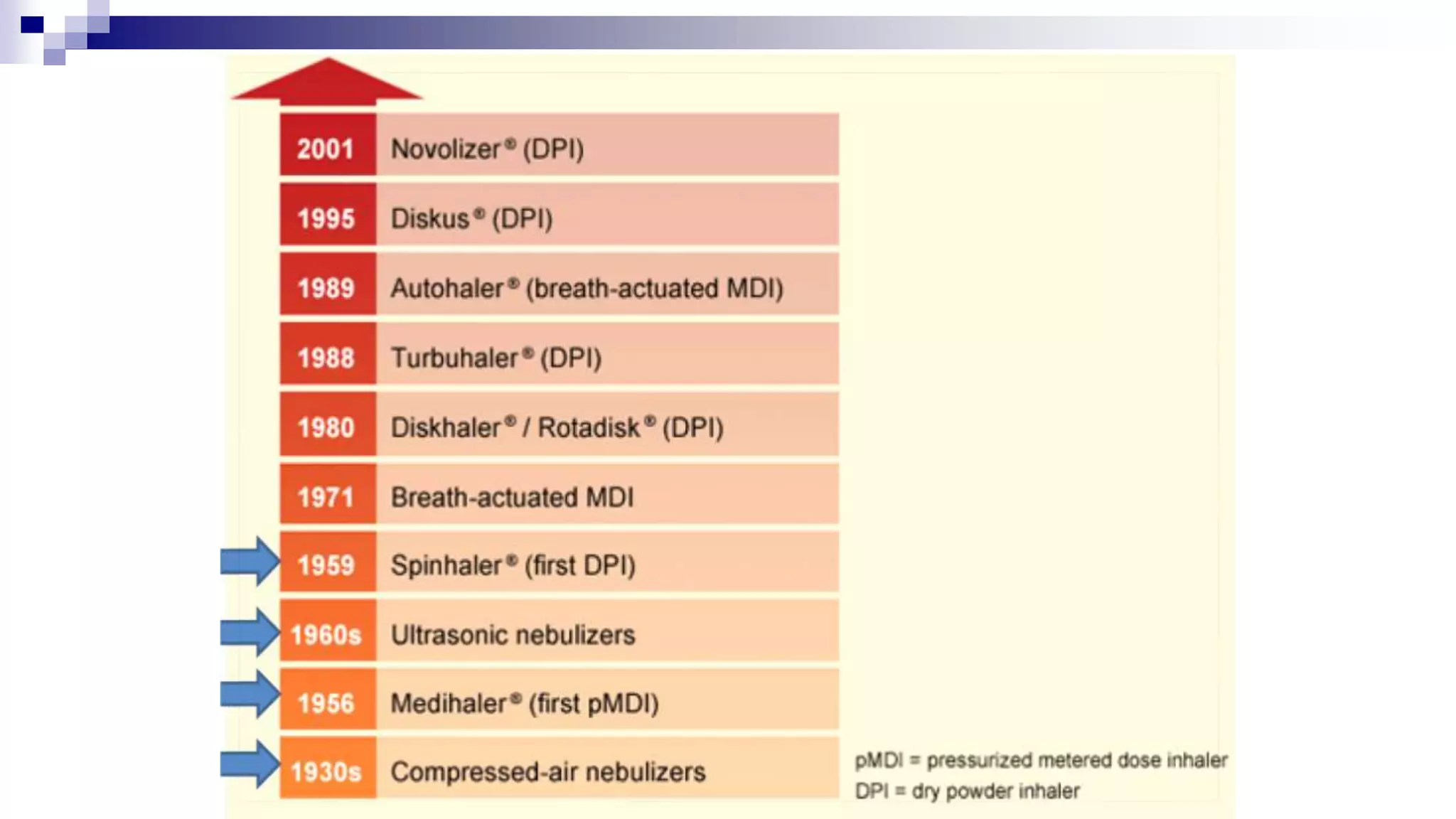
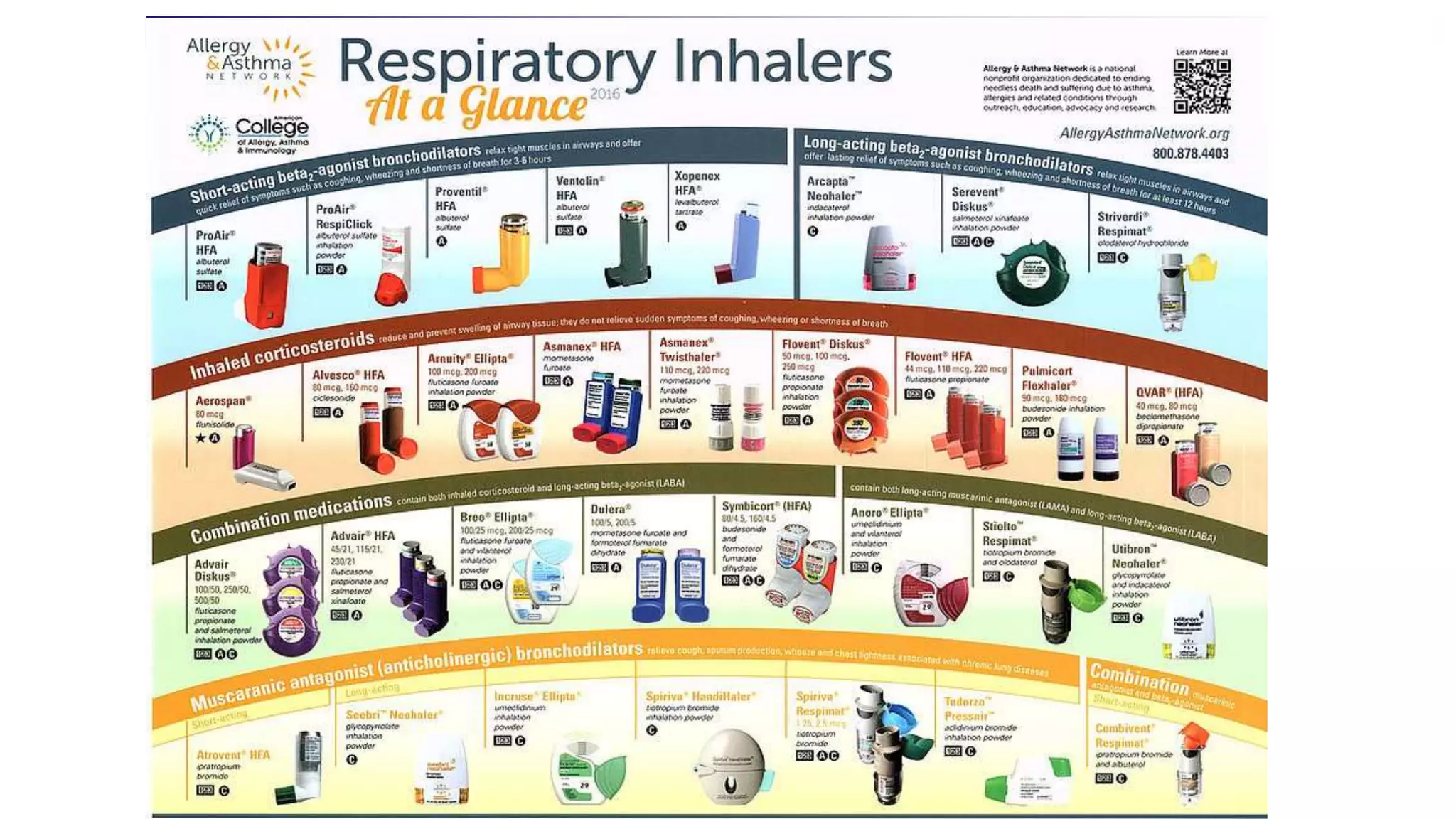
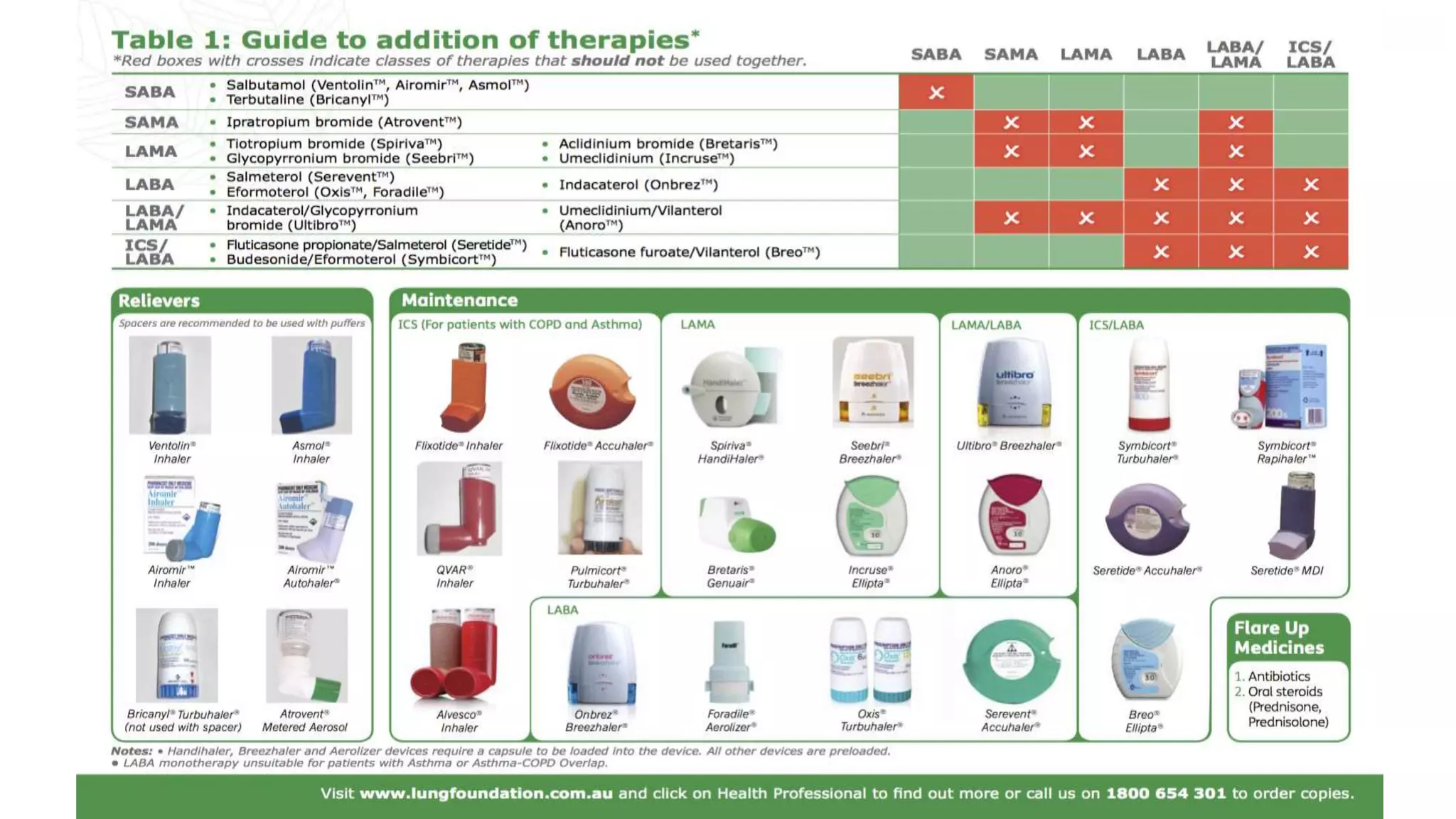
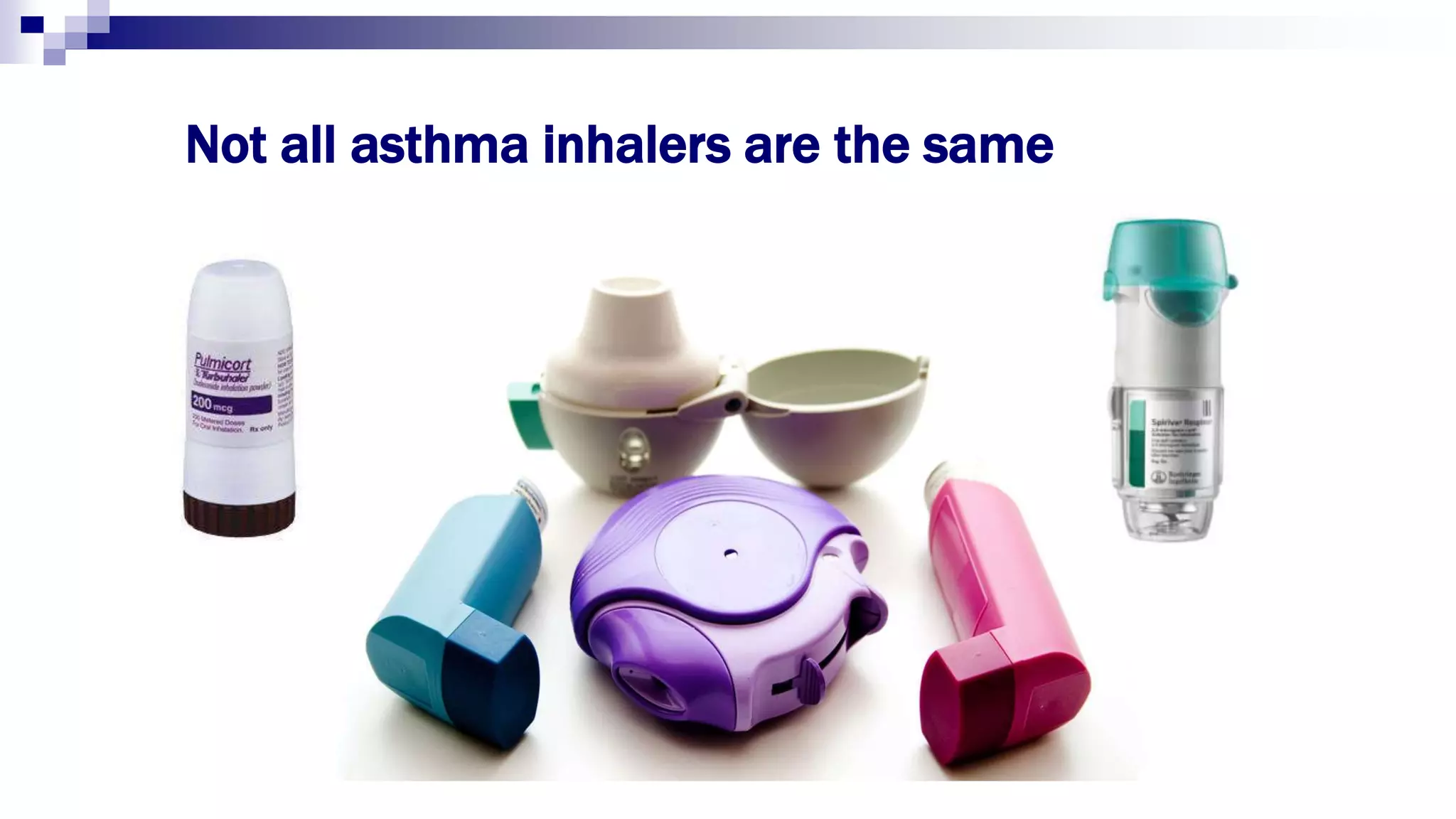
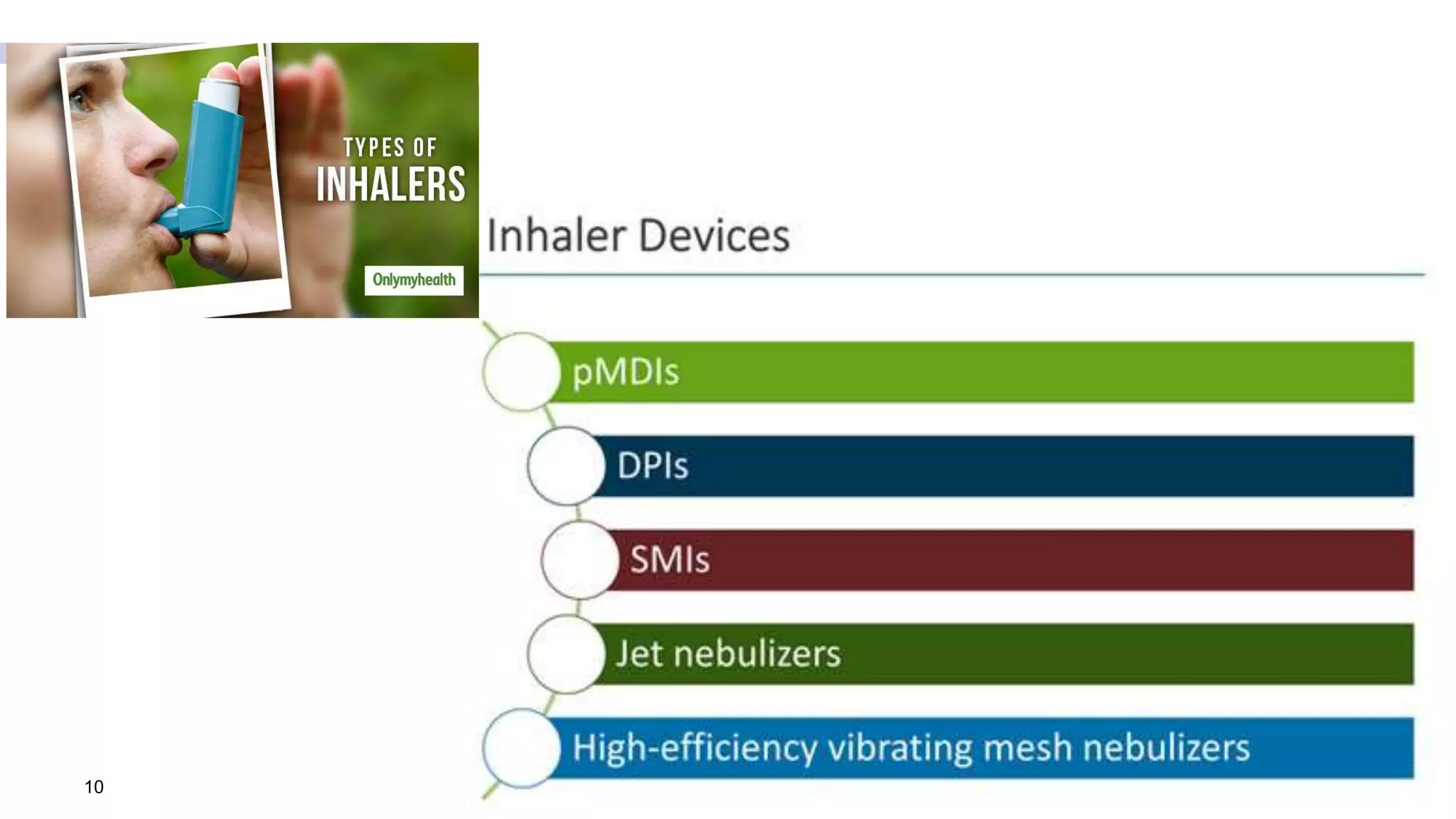
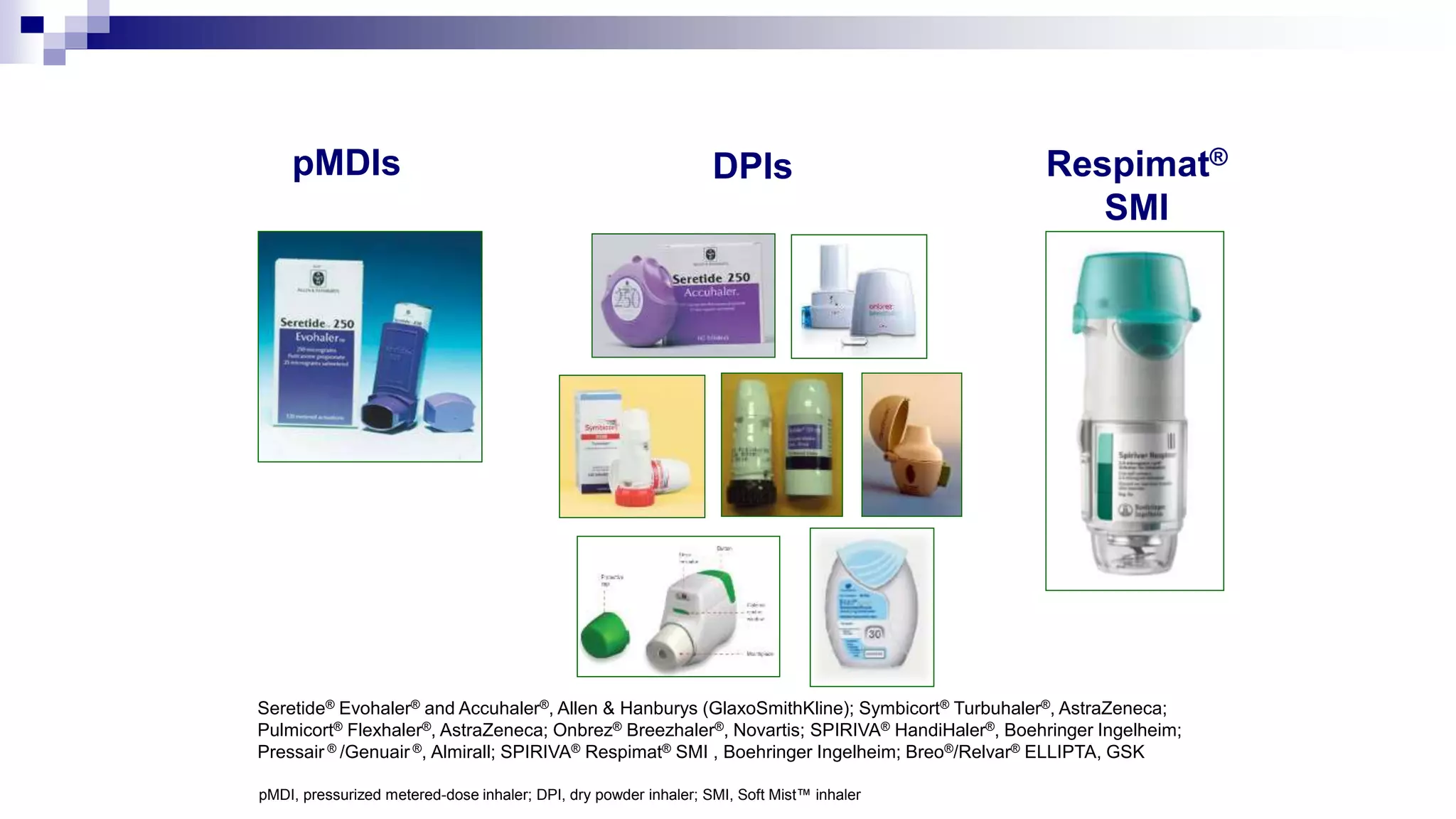


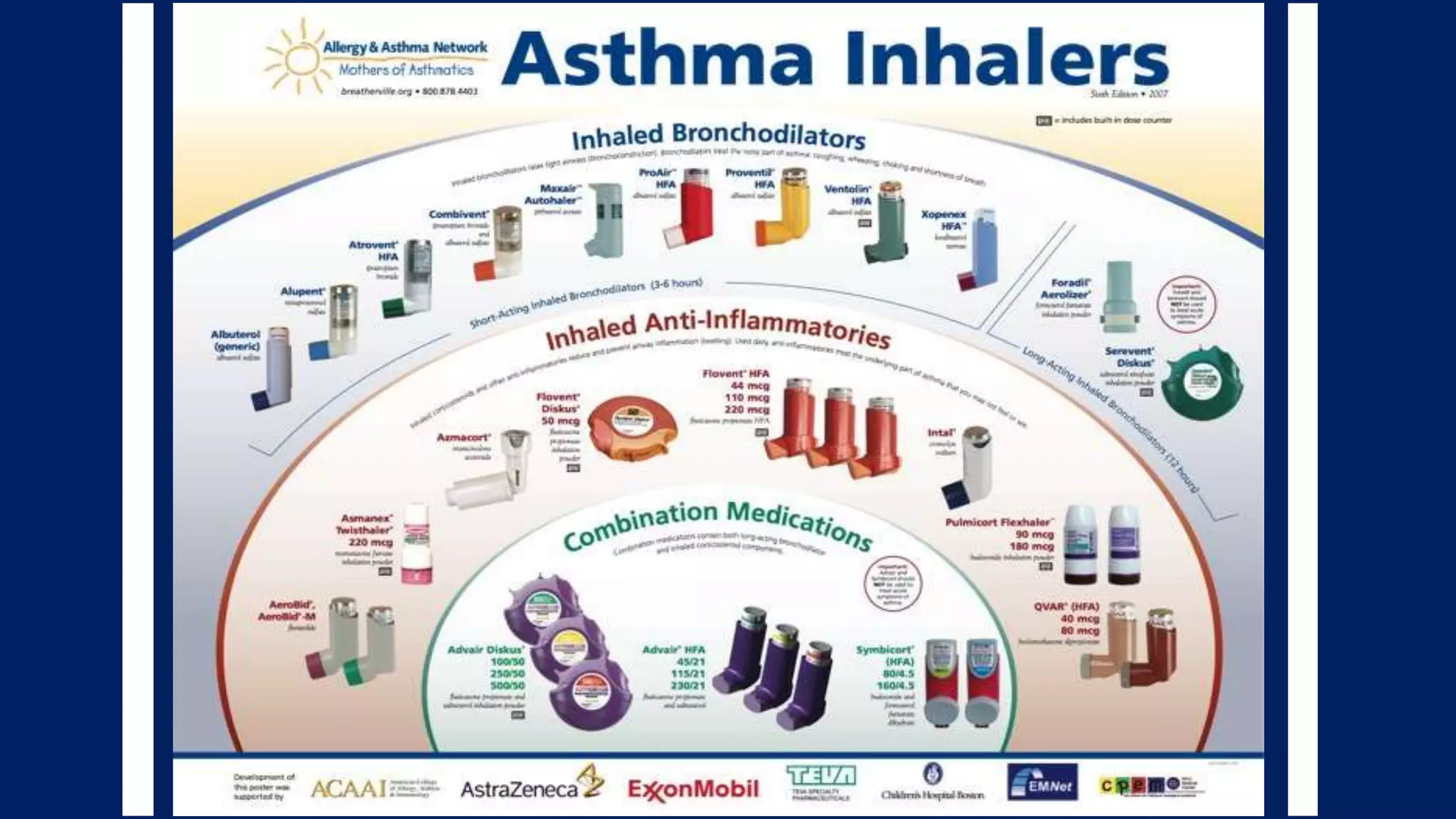
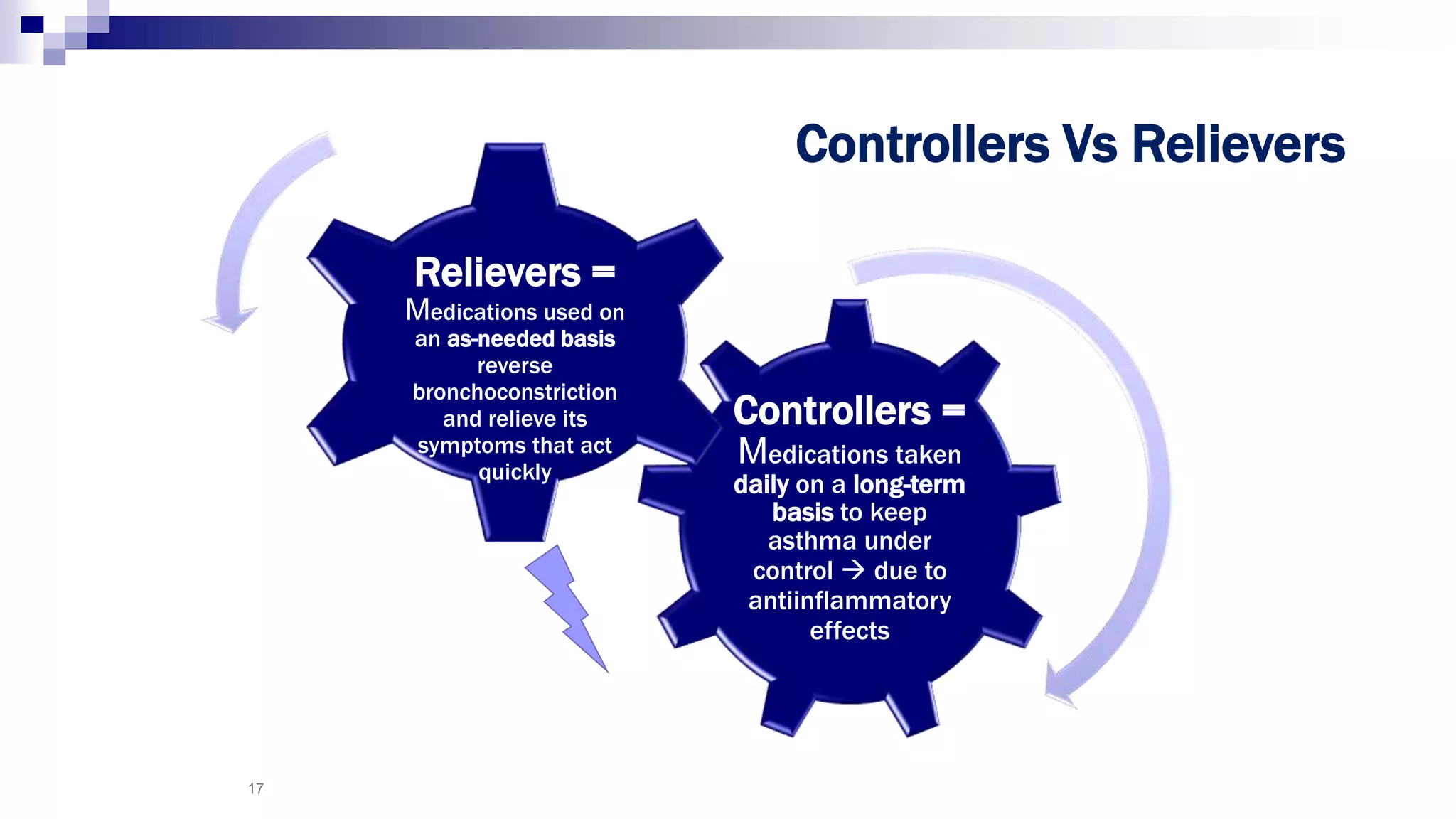
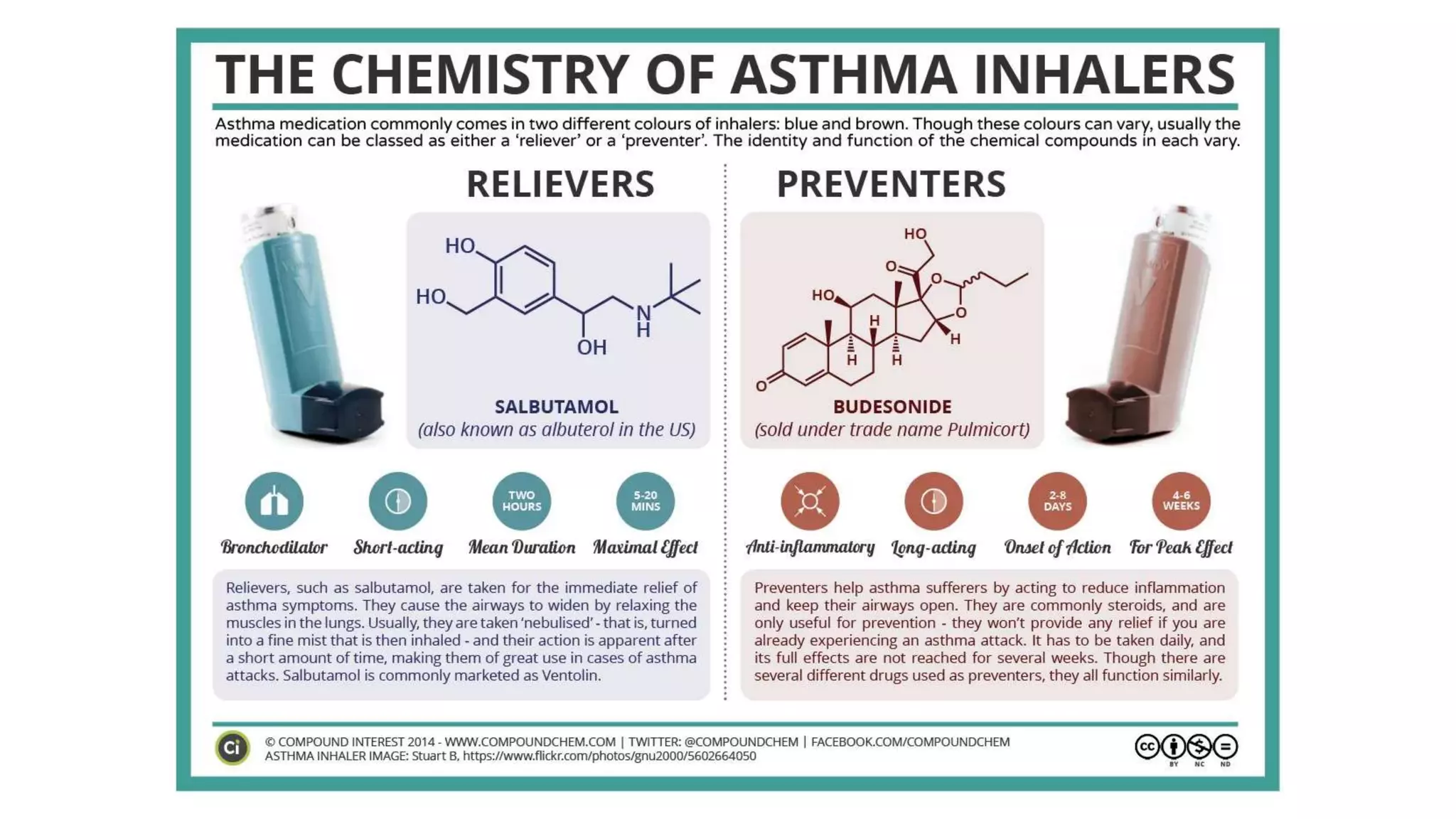

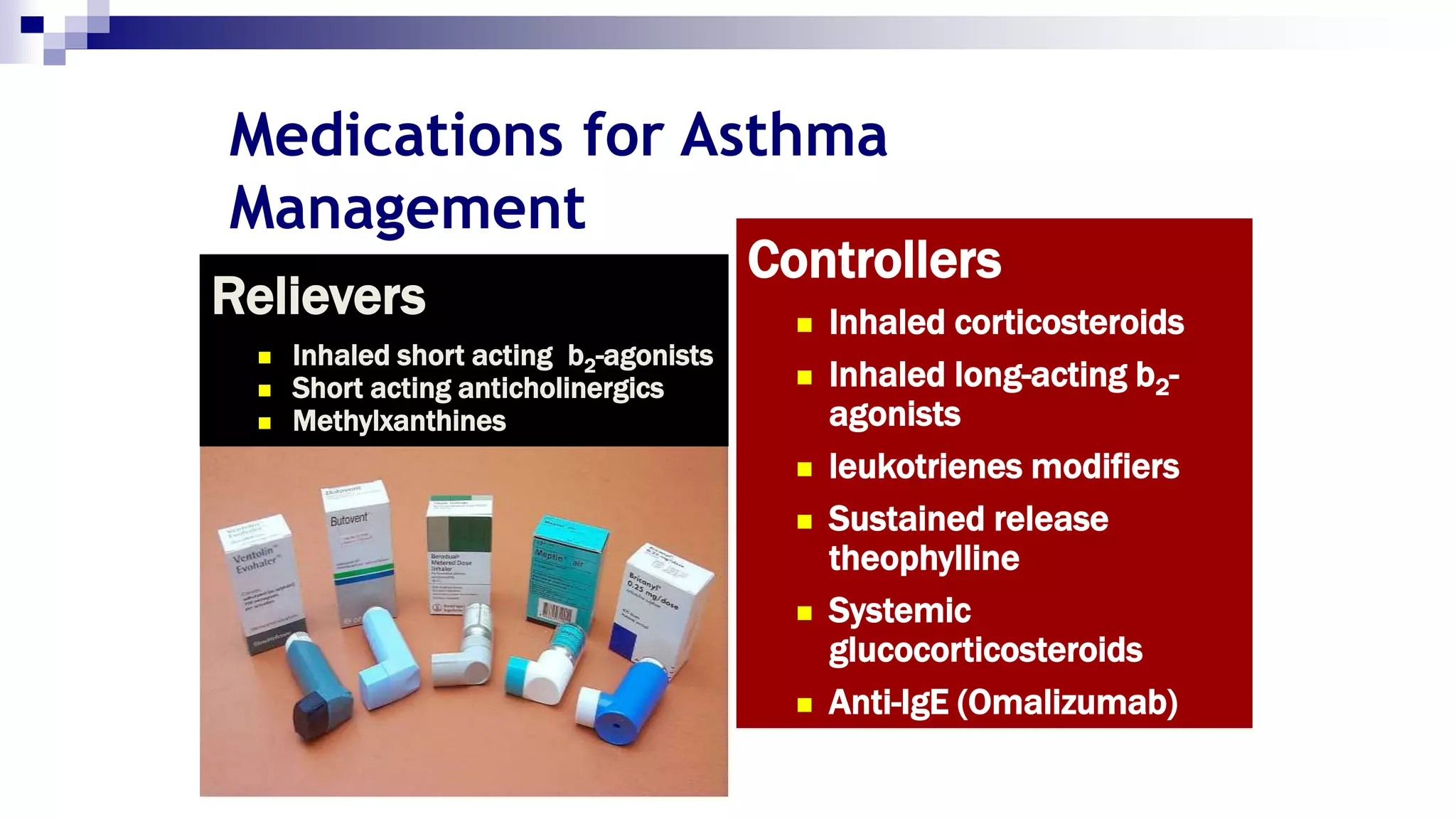




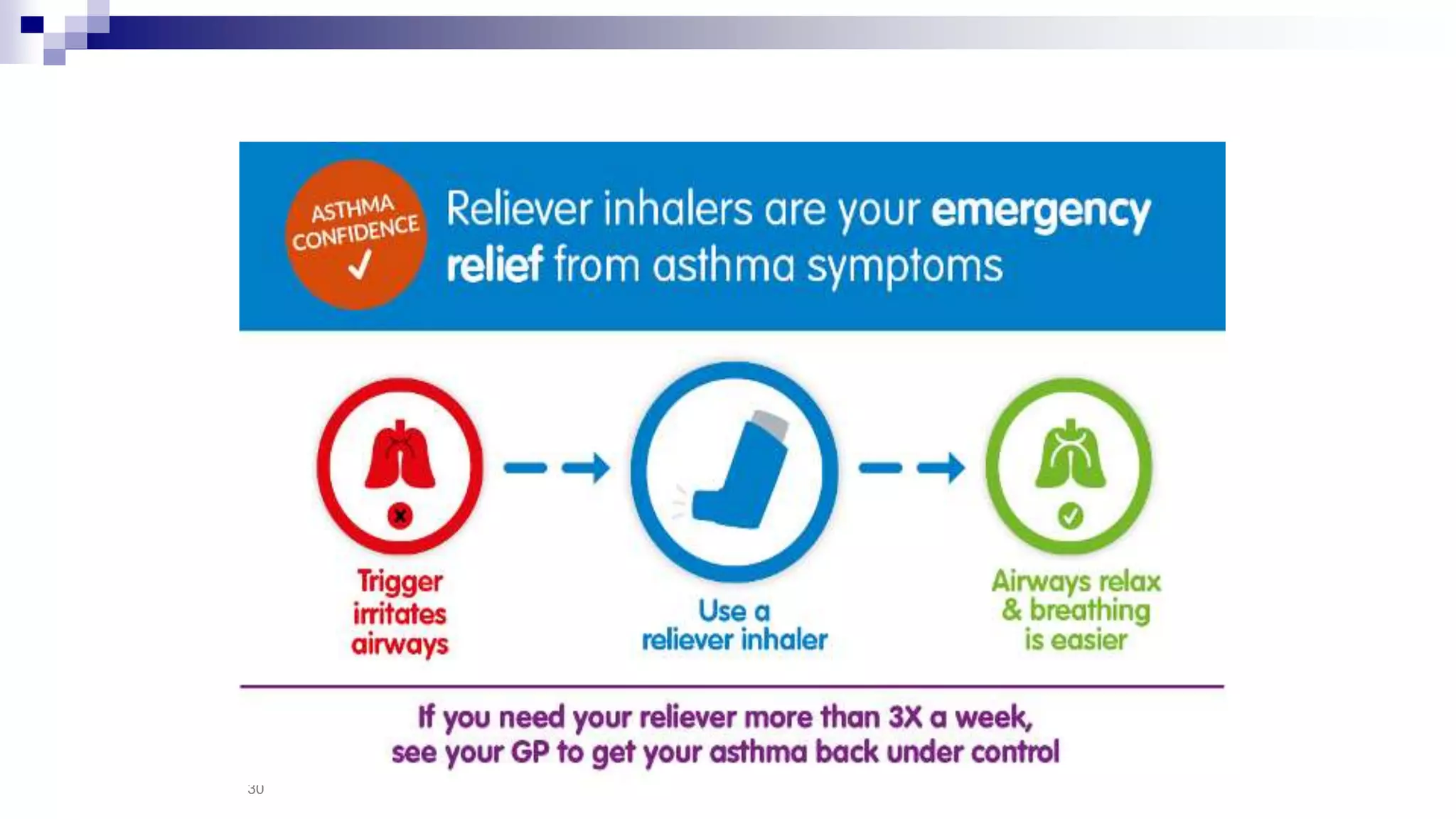


























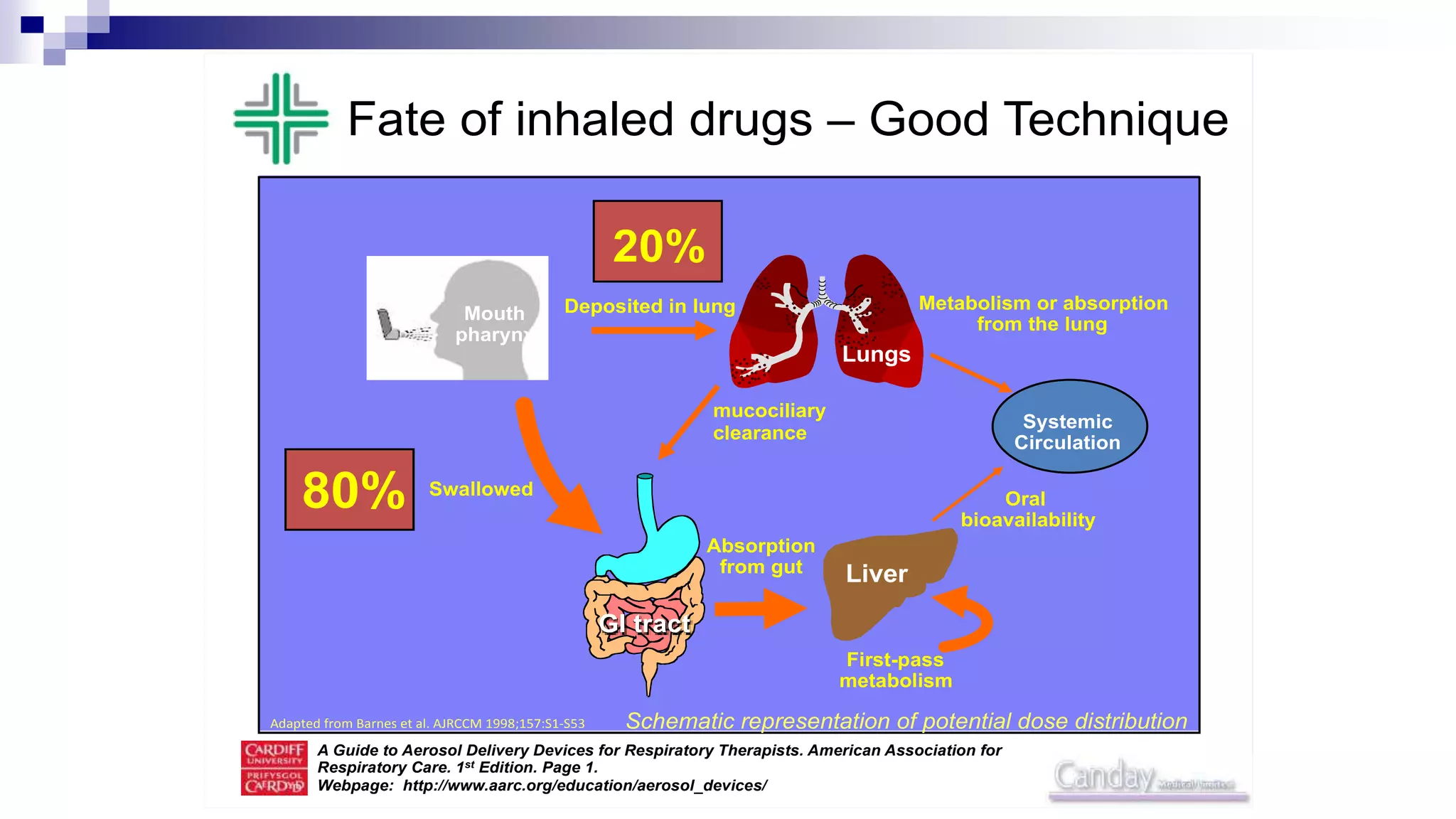
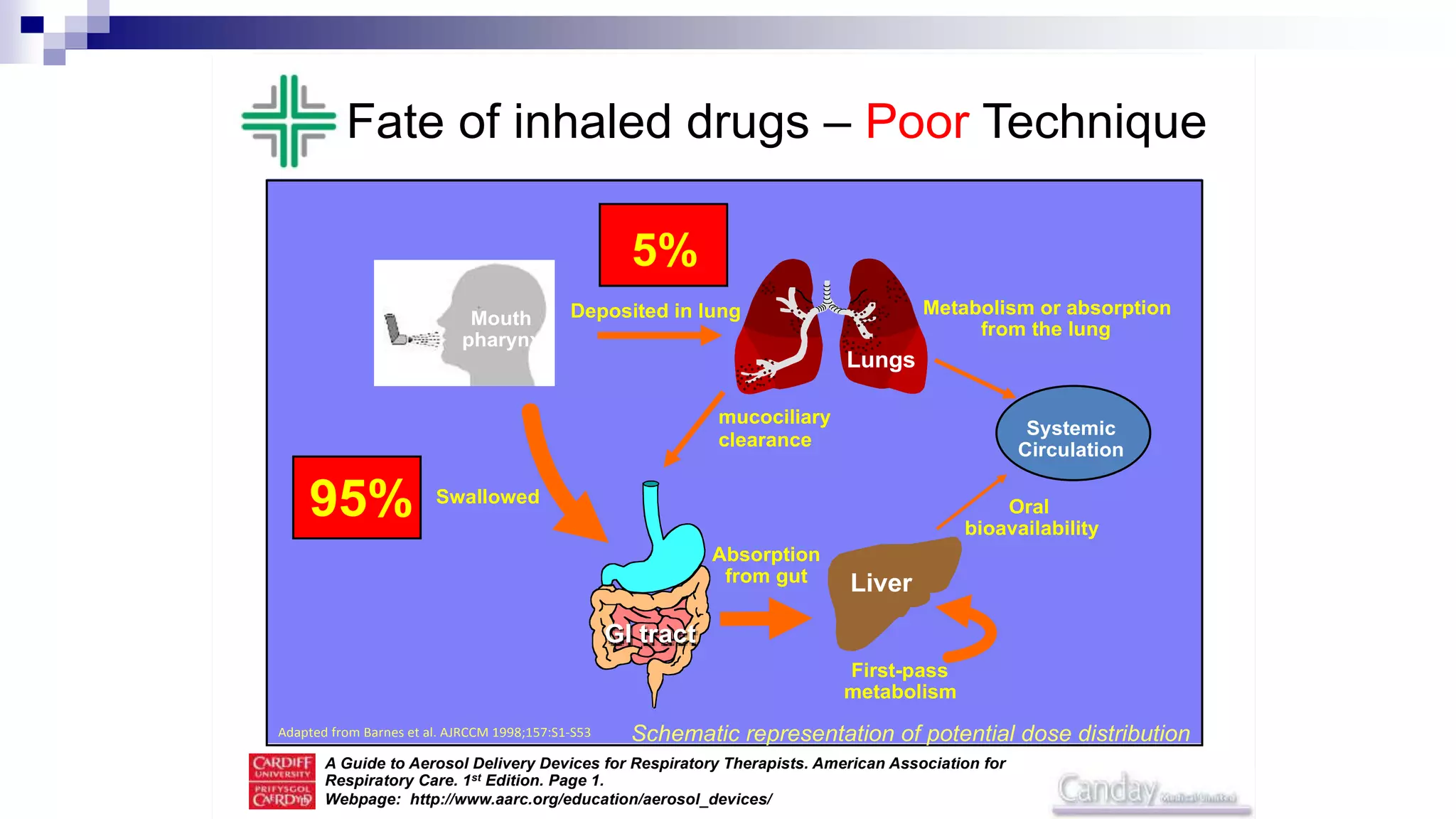




This document provides an overview of inhaled therapy for asthma. It discusses the history of inhaled treatments and different types of inhalers. The key aspects covered include: - Inhaled therapy is the cornerstone of asthma treatment and works by directly delivering medication to the airways. - Different types of inhalers include pressurized metered dose inhalers, dry powder inhalers, and soft mist inhalers. - Inhaled medications are divided into controllers taken daily to control inflammation and relievers used as needed to provide quick symptom relief. - Proper inhaler technique is important for effective delivery of medication to the lungs.





![Newer drugs in management of copd [2018 update]](https://cdn.slidesharecdn.com/ss_thumbnails/newerdrugsinmanagementofcopd2018update-180309071249-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































