Downloaded 89 times























































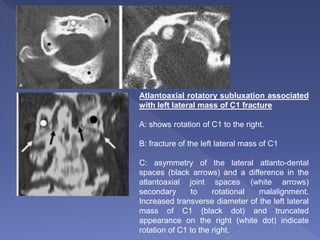































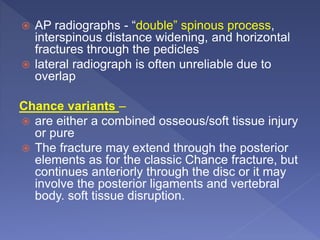







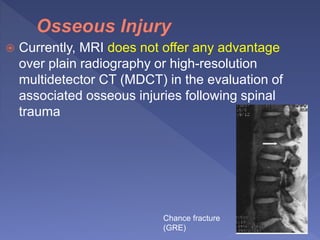













This document discusses spinal trauma, with a focus on cervical spine injuries. It provides details on: - Epidemiology of spinal cord injuries and common causes - Imaging techniques used to evaluate spinal trauma, including radiography, CT, MRI - Clinical criteria like NEXUS and Canadian C-Spine Rule that can determine if imaging is needed - Differences in cervical spine injuries between age groups and considerations for imaging children - Types of fractures more common in the elderly - Using CT to evaluate the thoracolumbar spine - Advantages and limitations of various imaging modalities and techniques































































































