Downloaded 609 times





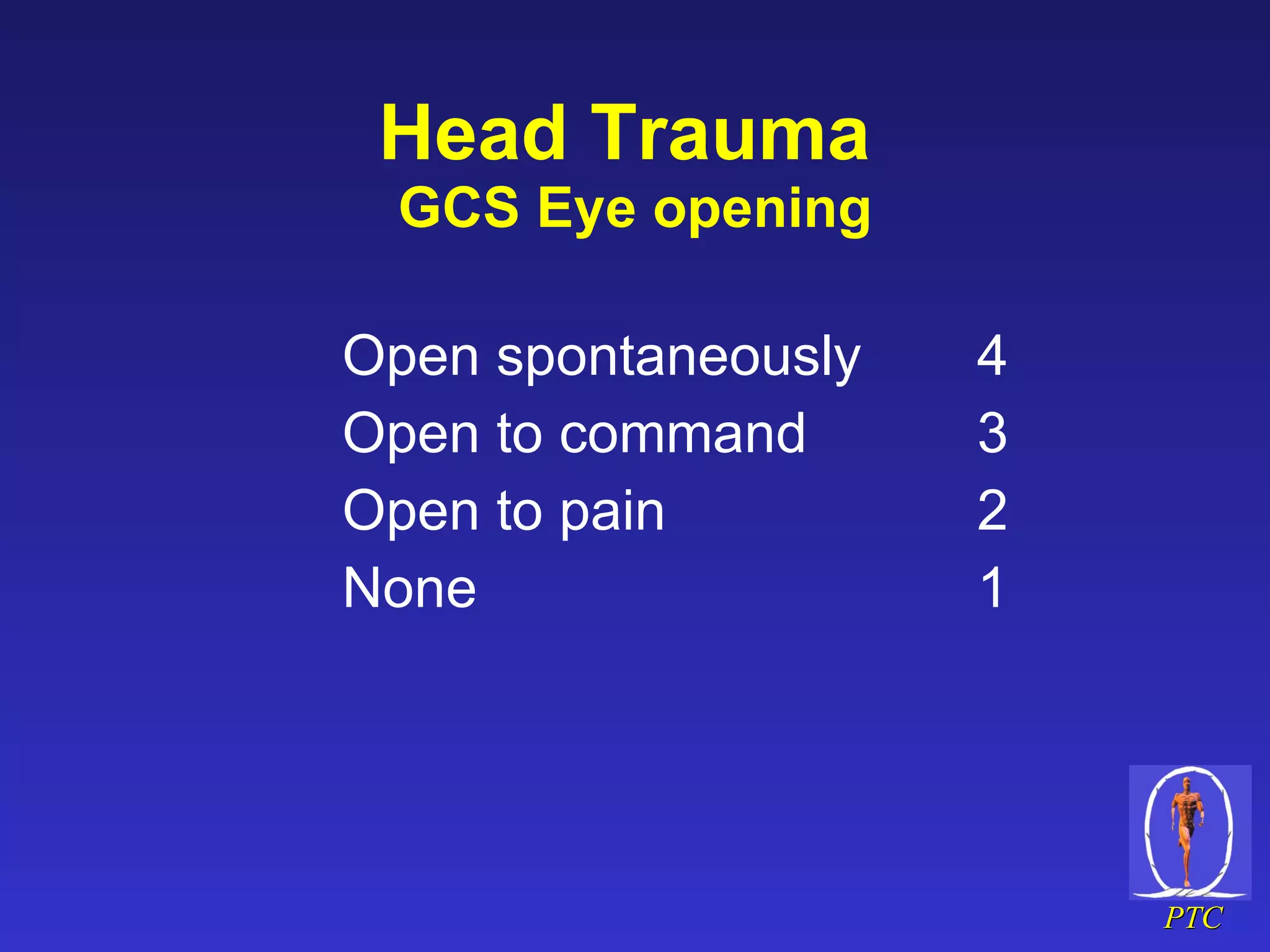



















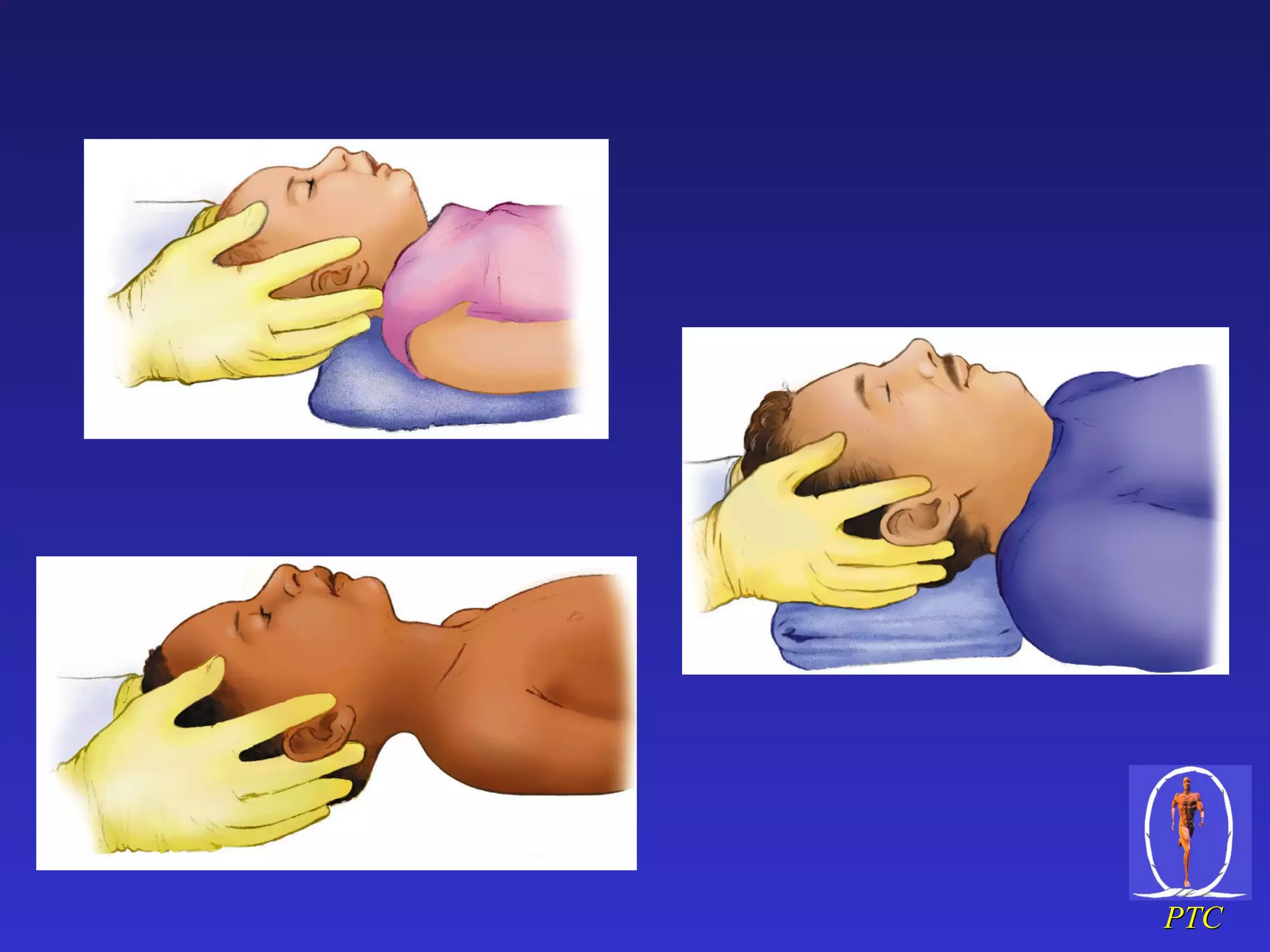





























The document provides information on the assessment and management of head and spinal trauma. It outlines the ABC approach for head trauma and emphasizes preventing secondary brain injury. It describes evaluating the Glasgow Coma Scale and pupillary responses. For spinal trauma, it stresses immobilization and protecting the spine during transport. Key factors include preventing further neurological injury and addressing airway, breathing, circulation issues.



































































