Downloaded 430 times

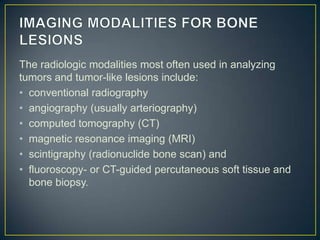
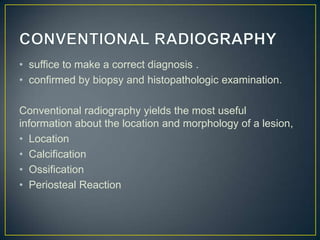








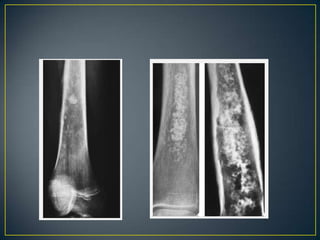










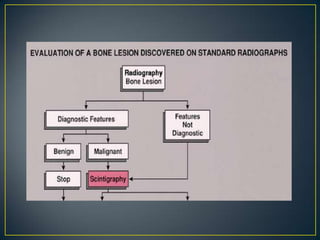
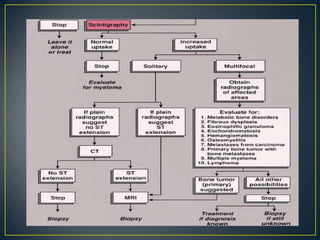


This document discusses various imaging modalities used to analyze bone tumors, including their benefits and limitations. Conventional radiography is still the standard first technique used to determine location, morphology, and suspicious findings. Based on radiography results, further imaging such as CT, MRI, scintigraphy, or angiography may be used to better evaluate tumor extent, involvement of surrounding tissues, and vascular supply. Each additional technique provides more detailed information but also has advantages and disadvantages depending on the tumor characteristics and goals of assessment. Together, imaging tests help diagnose and plan treatment of bone tumors.























































































