Downloaded 1,732 times




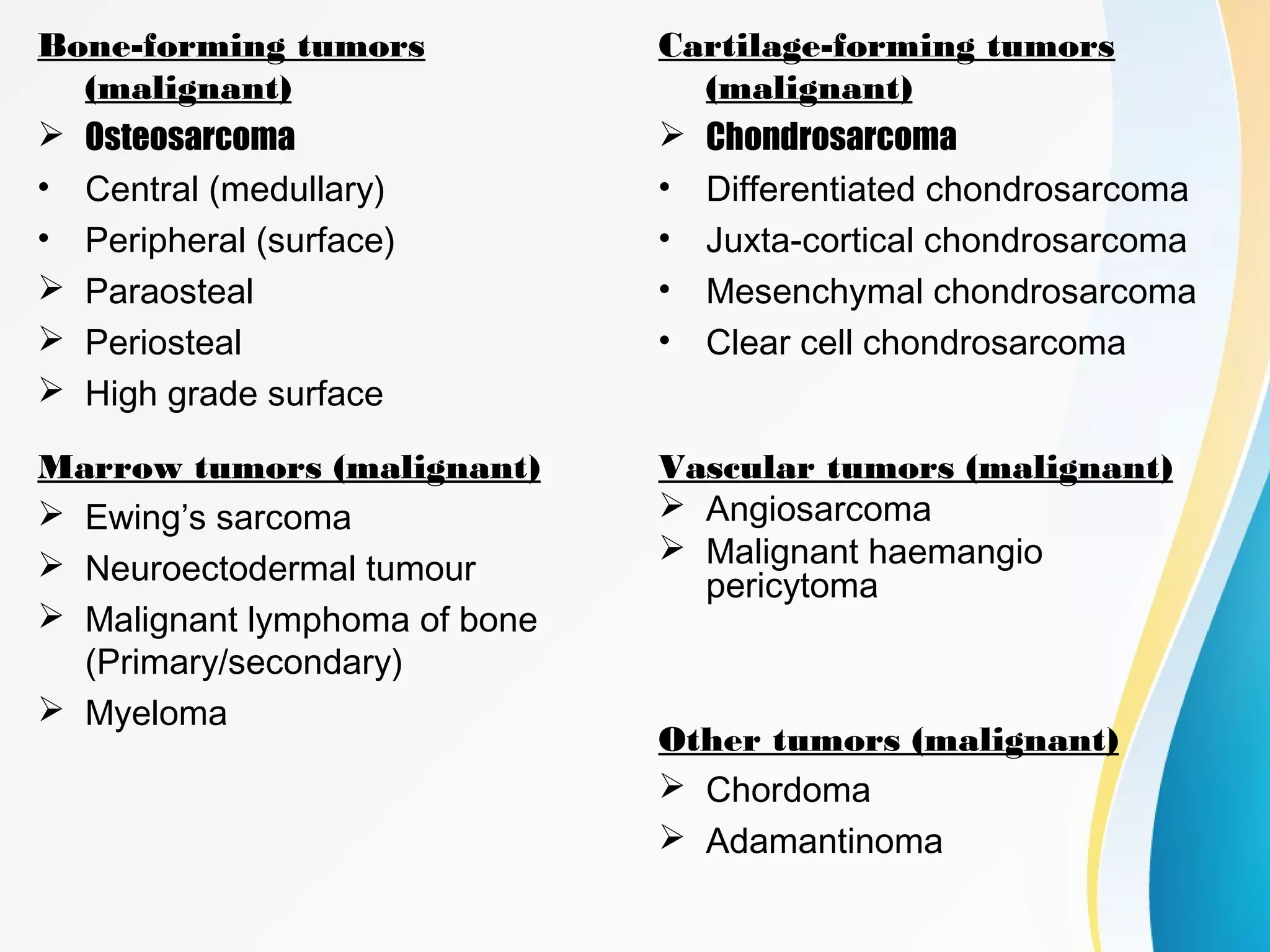






















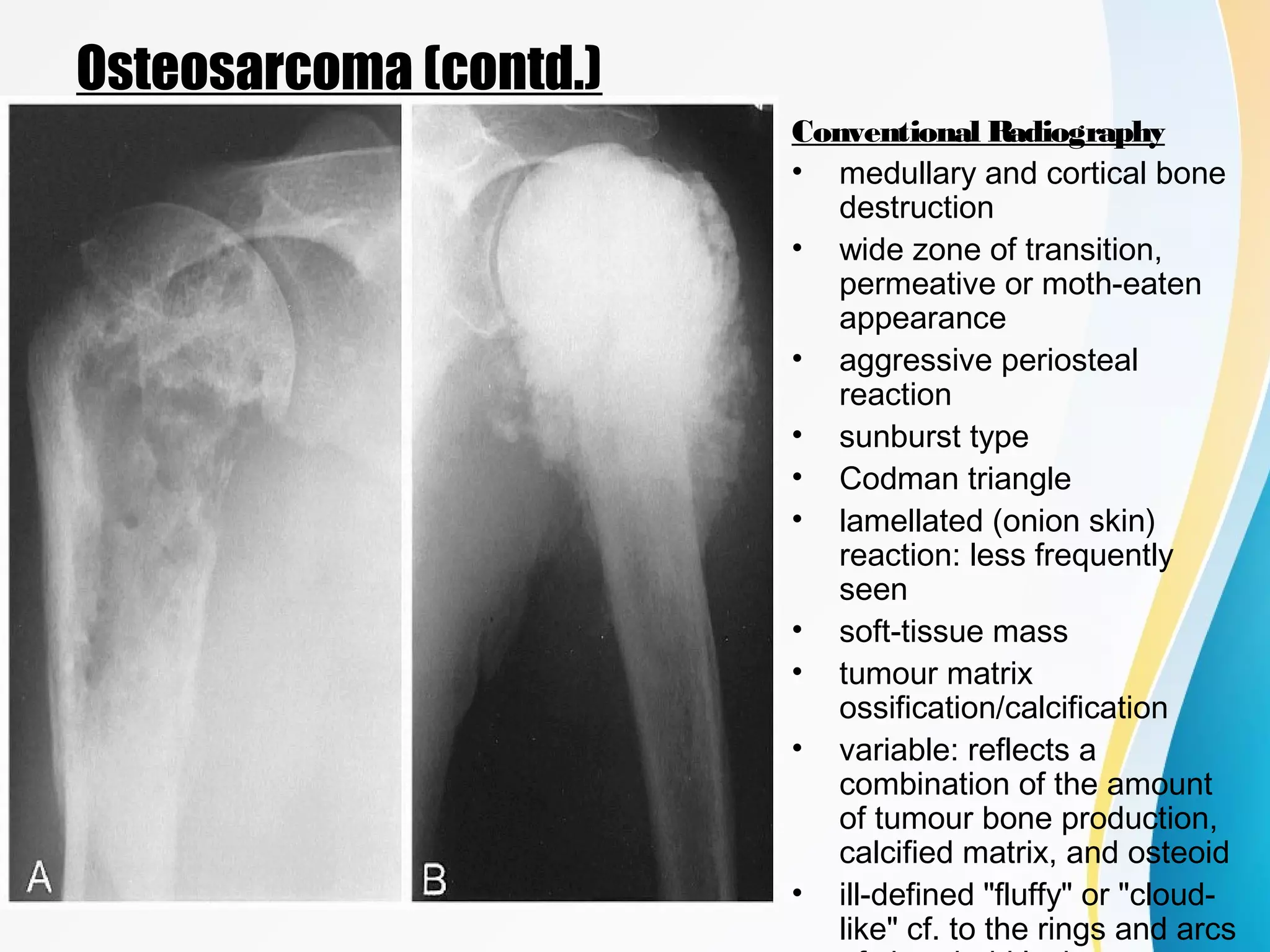

























This document provides an overview of malignant bone tumors, including their classification, occurrence, imaging appearance, and examples. It discusses several primary malignant bone tumors in detail, including osteosarcoma and multiple myeloma. Osteosarcoma most commonly affects teenagers and young adults, presents as aggressive bone destruction with periosteal reaction on x-ray, and has variable appearances on MRI/CT. Multiple myeloma commonly affects older adults, causes lytic lesions scattered throughout the skeleton appearing as "punched out" areas on x-ray, and MRI is most sensitive for detecting its bone involvement. The document outlines radiographic features that can help characterize and differentiate various malignant bone tumors.























































































