This document provides an overview of pharmacology concepts including:
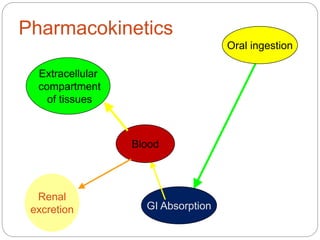
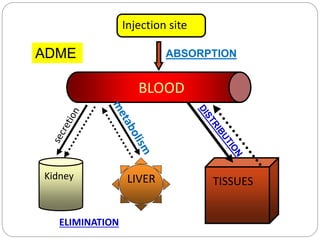
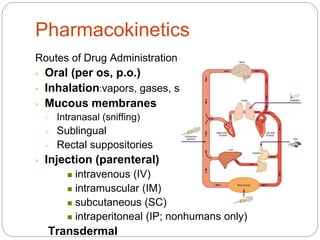
- Pharmacokinetics describes what the body does to drugs through absorption, distribution, metabolism and excretion.
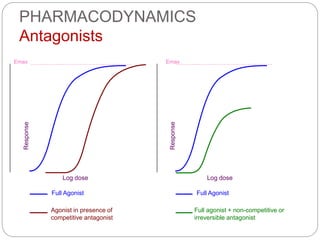
- Pharmacodynamics describes what drugs do to the body through receptor interactions and clinical effects.
- Key pharmacokinetic processes like absorption, distribution, metabolism and elimination are influenced by drug and body factors and determine drug availability at target sites.




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
