Downloaded 334 times

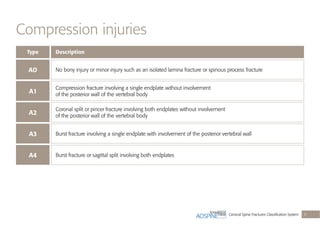
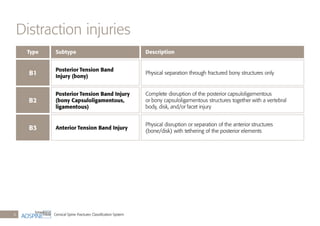

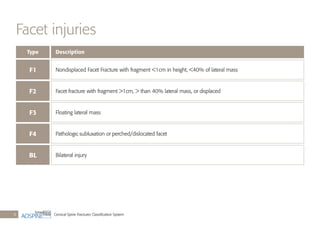
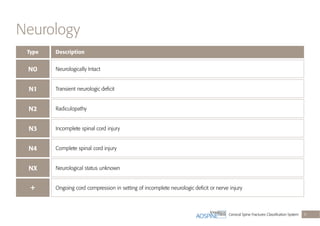
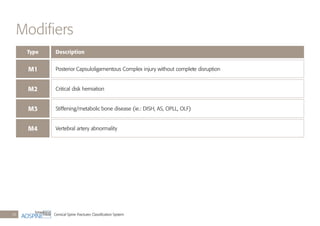
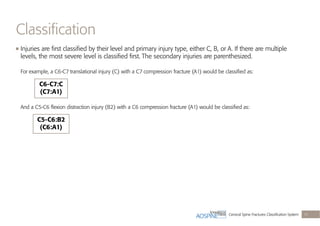

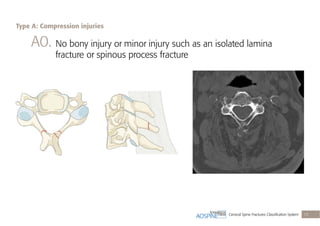
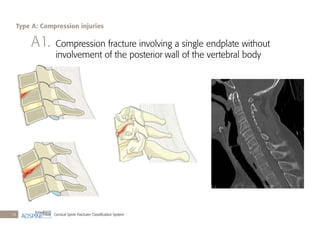
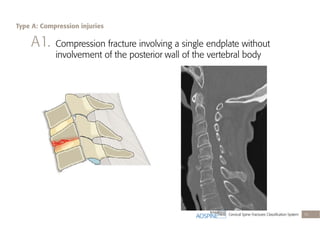
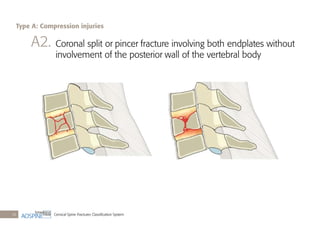
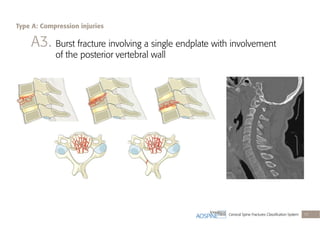
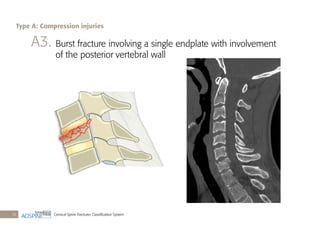
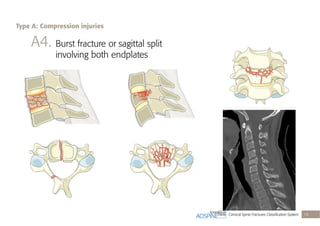
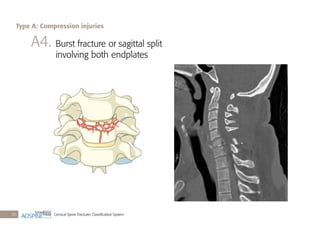
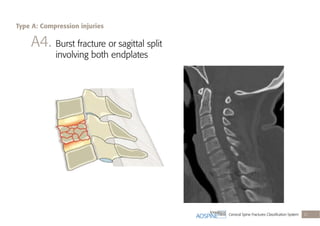
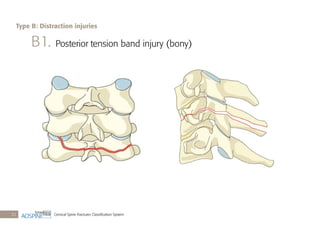
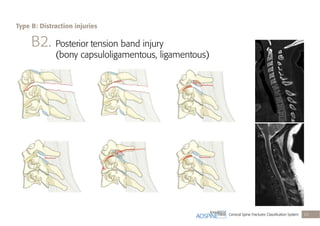
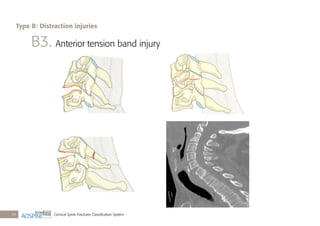
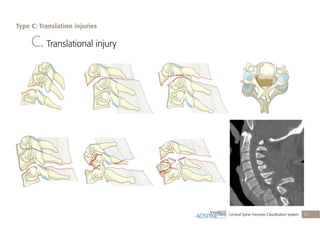
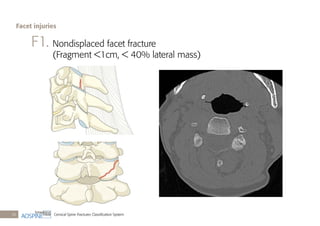
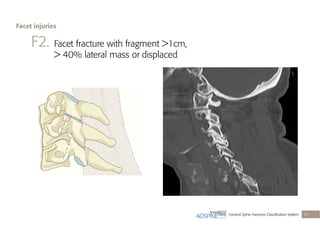
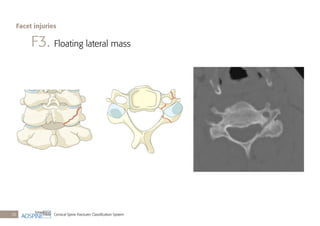
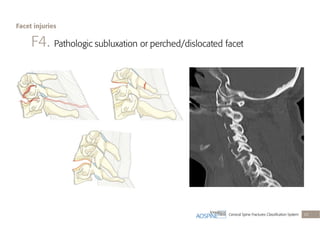
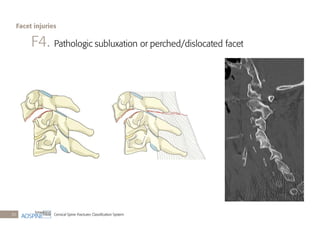
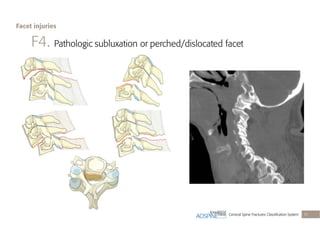
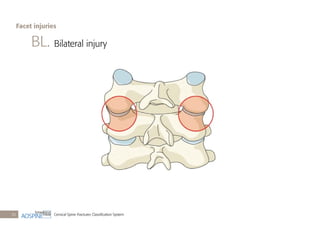
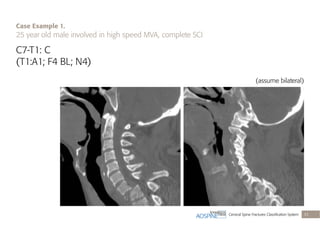

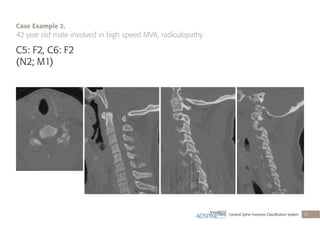
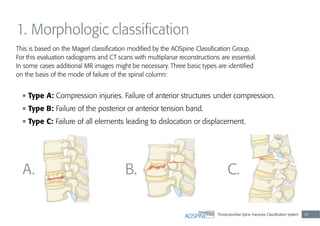
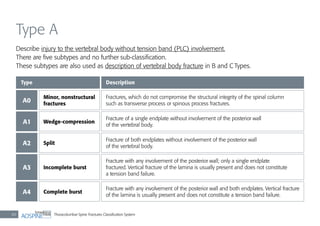
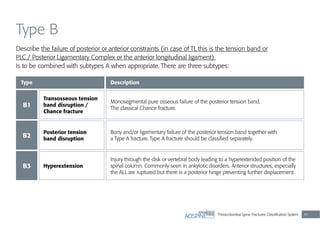

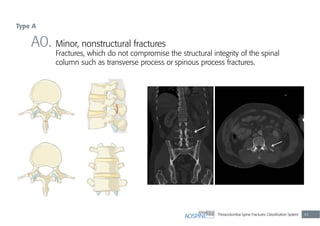
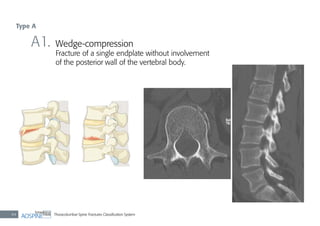
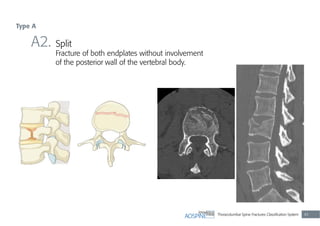
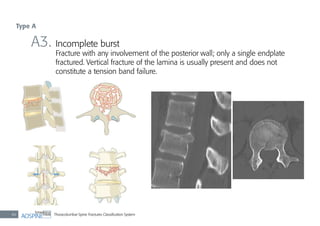
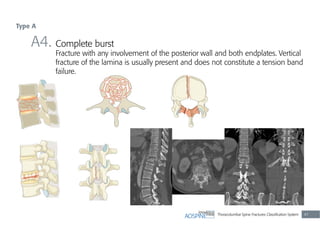
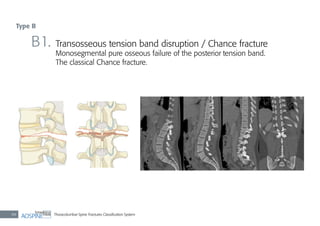
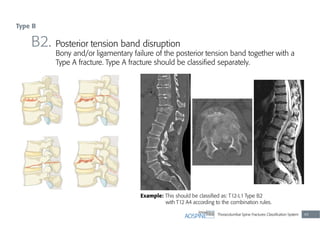
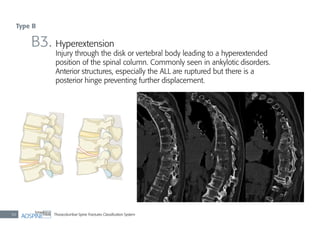
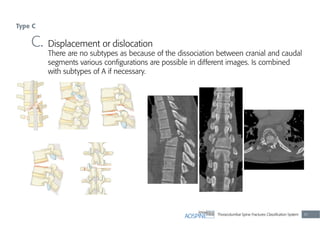
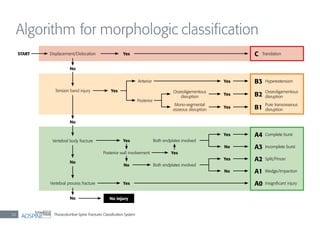
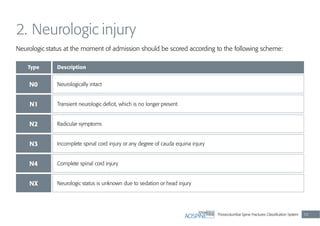
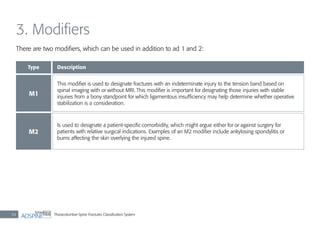


This document presents a classification system for spinal fractures developed by AOSpine. It includes: - Classification of cervical spine fracture types A-C, including compression (A), distraction (B), and translation (C) injuries. It also covers facet injuries and neurological status. - Descriptions and illustrations of each fracture type (A1-A4, B1-B3, etc.) along with case examples. - The goal is to develop a standardized system that can be used for research and guide treatment of spinal fractures. The system is being scientifically validated before potential adoption as the official AOSpine classification.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















